You might also like
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
- Al-Bayan University Pharmacy College 3 Stage: Lecture 8 Pharmacology Antibiotics DR - Khulood SaadoonDocument19 pagesAl-Bayan University Pharmacy College 3 Stage: Lecture 8 Pharmacology Antibiotics DR - Khulood SaadoonAhmed HadeerNo ratings yet
- Antibacterial: Topics: 1. Cell Wall Synthesis InhibitorDocument26 pagesAntibacterial: Topics: 1. Cell Wall Synthesis InhibitorMusfira YaseenNo ratings yet
- Antibacterial Drugs Cellwall and Protein Synthesis InhihibitorsDocument41 pagesAntibacterial Drugs Cellwall and Protein Synthesis InhihibitorsWezzyNo ratings yet
- Antimicrobial Therapy: A) Anti-BacterialDocument9 pagesAntimicrobial Therapy: A) Anti-BacterialUnor KnownNo ratings yet
- Lac 10&11 PPTDocument16 pagesLac 10&11 PPTRaghdaNo ratings yet
- Antibiotics - PenicillinsDocument14 pagesAntibiotics - PenicillinsDheemanth veerlaNo ratings yet
- Penicillins 1Document30 pagesPenicillins 1John PaulNo ratings yet
- Cep Halo Sporin SDocument51 pagesCep Halo Sporin Smonir61No ratings yet
- NotesDocument9 pagesNotesVivianNo ratings yet
- Beta Lactum AntibioticsDocument26 pagesBeta Lactum AntibioticsEmon KhanNo ratings yet
- Phar - Cell Wall Inhibitor - Lec 7 - TheoDocument20 pagesPhar - Cell Wall Inhibitor - Lec 7 - Theoسلام شاكر حميد جميل 6506No ratings yet
- Introduction To Beta Lactam AntibioticsDocument31 pagesIntroduction To Beta Lactam AntibioticsVishaal BhatNo ratings yet
- PenicillinDocument21 pagesPenicillinnadar shahNo ratings yet
- AntibioticsDocument51 pagesAntibioticsClarenceNo ratings yet
- Beta Lactam AntibioticsDocument28 pagesBeta Lactam AntibioticsHassan.shehri100% (11)
- ChemotherapyDocument11 pagesChemotherapyNedaAbdullahNo ratings yet
- Chemo For LabDocument117 pagesChemo For Labsinte beyuNo ratings yet
- Antibacterials and AntibioticsDocument44 pagesAntibacterials and AntibioticsVallejo Taberna HannalieNo ratings yet
- Pharmacology: Classification and Mode of Action of AntibioticsDocument44 pagesPharmacology: Classification and Mode of Action of AntibioticsAamir AzizNo ratings yet
- 2-Cell Wall Inhibitor Antibitics-I Oct 15th 2018Document28 pages2-Cell Wall Inhibitor Antibitics-I Oct 15th 2018Leena AlateeqNo ratings yet
- AntibioticsDocument5 pagesAntibioticsSneeha VeerakumarNo ratings yet
- Lecture 11 - 306-Antimicrobial - QDocument19 pagesLecture 11 - 306-Antimicrobial - QFaysal HassanNo ratings yet
- Antibiotics CologyDocument31 pagesAntibiotics CologyManthan ChauhanNo ratings yet
- Final Exam PointersDocument53 pagesFinal Exam PointersBelleNo ratings yet
- Antibiotic Resistance: Dr. Sharifah Shakinah Supervisor: Dr. Eppy SPPD KptiDocument25 pagesAntibiotic Resistance: Dr. Sharifah Shakinah Supervisor: Dr. Eppy SPPD KptiShasha Shakinah100% (1)
- Chemotherapy AntibioticsDocument23 pagesChemotherapy AntibioticsMubarak Abubakar yaroNo ratings yet
- Chemotherapeutic Agent: Bacteria Synonymously Antimicrobial AntifungalDocument5 pagesChemotherapeutic Agent: Bacteria Synonymously Antimicrobial AntifungalBrendo TorresNo ratings yet
- Mechanism of Action of Penicillin & CephalosporinDocument7 pagesMechanism of Action of Penicillin & CephalosporinshahabahmadNo ratings yet
- Antibiotics: Cephalosporins Mechanism and ClassificationDocument7 pagesAntibiotics: Cephalosporins Mechanism and ClassificationAhmed BajahNo ratings yet
- AntibioticsDocument21 pagesAntibioticsJerry ArockeNo ratings yet
- Introduction To Antimicrobials Page 1 of 6Document6 pagesIntroduction To Antimicrobials Page 1 of 6Hassan.shehriNo ratings yet
- Chapter-9 Antibiotic and Emergence of Resistance - 1Document27 pagesChapter-9 Antibiotic and Emergence of Resistance - 1Hillani TadesseNo ratings yet
- Penicillins: Classification, Mechanism of Action & UsesDocument58 pagesPenicillins: Classification, Mechanism of Action & UsesSally PujaNo ratings yet
- Principles of Antibiotics: Understanding How They WorkDocument117 pagesPrinciples of Antibiotics: Understanding How They WorkDeepa VenkateshNo ratings yet
- 11 Antiobiotics, Antifungals, and AntiviralsDocument16 pages11 Antiobiotics, Antifungals, and AntiviralseNo ratings yet
- Biology Lab Report AntibioticsDocument8 pagesBiology Lab Report AntibioticsLoore Liflander100% (1)
- Chemotherapy Agents for Bacterial InfectionsDocument18 pagesChemotherapy Agents for Bacterial InfectionsShubhendu ChattopadhyayNo ratings yet
- Pharma BDocument6 pagesPharma BKatrina EstoconingNo ratings yet
- AntibioticsDocument8 pagesAntibioticsمحمد بن صالحNo ratings yet
- Penicillins - KatzungDocument6 pagesPenicillins - KatzungKarl CNo ratings yet
- Cell Wall Synthesis Inhibitors: Pharmacology Seminar Group: A1Document113 pagesCell Wall Synthesis Inhibitors: Pharmacology Seminar Group: A1Lola KhatimNo ratings yet
- Chemotherapy Classification & AntibioticsDocument46 pagesChemotherapy Classification & AntibioticsErl D. Melitante100% (1)
- AntibioticsDocument69 pagesAntibioticsVidya Jayasekaran JNo ratings yet
- PenicillinsDocument23 pagesPenicillinsajpharmacist117No ratings yet
- East Timor Antibiotic Guidelines Jan17 PRINT v3Document114 pagesEast Timor Antibiotic Guidelines Jan17 PRINT v3Yoan Manuel Ruiz ArencibiaNo ratings yet
- Antimicrobials and Cytotoxic Drugs: DR Caroline Tetteyfio Koney 37 Military Hospital Accra Feb 2012Document58 pagesAntimicrobials and Cytotoxic Drugs: DR Caroline Tetteyfio Koney 37 Military Hospital Accra Feb 2012Fred OseiNo ratings yet
- AntibioticsDocument168 pagesAntibioticsamirabadr2005No ratings yet
- AntibioticsDocument10 pagesAntibioticsWendy VasquezNo ratings yet
- Antibiotics in EndodonticsDocument74 pagesAntibiotics in EndodonticsdrishyaNo ratings yet
- ANTIBIOTICS IN ORAL SURGERYs 123Document43 pagesANTIBIOTICS IN ORAL SURGERYs 123Puneet SinghNo ratings yet
- CLINICAL USE OF ANTIBIOTICS IN VETERINARY PRACTICEDocument83 pagesCLINICAL USE OF ANTIBIOTICS IN VETERINARY PRACTICEhansmeet100% (1)
- Beta Lactams 1Document44 pagesBeta Lactams 1C E princeyNo ratings yet
- Antibacterial and Antiinfective AgentsDocument80 pagesAntibacterial and Antiinfective AgentsAbbeygale GalanNo ratings yet
- Introduction To AntibioticsDocument12 pagesIntroduction To AntibioticsAlaa AhmedNo ratings yet
- Antibiotic 1-Terminology: 1. Inhibition of Cell Wall SynthesisDocument12 pagesAntibiotic 1-Terminology: 1. Inhibition of Cell Wall SynthesismidoNo ratings yet
- Week 3 & 4 AntimicrobialsDocument120 pagesWeek 3 & 4 AntimicrobialsQuerubin DandoyNo ratings yet
- Antibiotic Therapy GuideDocument5 pagesAntibiotic Therapy GuideFerreze AnnNo ratings yet
- Day 2 General Microbiology 12-1-2021Document150 pagesDay 2 General Microbiology 12-1-2021ShriefElghazalyNo ratings yet
- PenicillinDocument8 pagesPenicillinVaagi LogiNo ratings yet
- Guideline FullDocument61 pagesGuideline FullvexicaNo ratings yet
- The Clinical and Immunological Features of Leprosy: S. L. Walker and D. N. J. LockwoodDocument19 pagesThe Clinical and Immunological Features of Leprosy: S. L. Walker and D. N. J. LockwoodvexicaNo ratings yet
- Vancouver Citation Style GuideDocument7 pagesVancouver Citation Style GuideGerardo Alberto Padilla MartínezNo ratings yet
- WHO Dengue Guidelines 2013Document160 pagesWHO Dengue Guidelines 2013Jason MirasolNo ratings yet
- Pathogenesis of LeprosyDocument13 pagesPathogenesis of LeprosyNurul AinNo ratings yet
- Ballard ScoreDocument1 pageBallard ScoreFikriyah FuadiyahNo ratings yet
- Central Venous Surgical Catheter or Long Line, Management of A Baby With PDFDocument16 pagesCentral Venous Surgical Catheter or Long Line, Management of A Baby With PDFvexicaNo ratings yet
- PPS - Revised Dengue Guidelines Fluid Management Oct 2012Document22 pagesPPS - Revised Dengue Guidelines Fluid Management Oct 2012lovelots1234100% (3)
- Ballard ScoreDocument1 pageBallard ScoreFikriyah FuadiyahNo ratings yet
- Staging of Lung CancerDocument14 pagesStaging of Lung CancervexicaNo ratings yet
- Indonesia TB ProfileDocument4 pagesIndonesia TB ProfilevexicaNo ratings yet
- Data Dan Output Oneway AnovaDocument4 pagesData Dan Output Oneway AnovaAdi SucandraNo ratings yet
- IHKDocument2 pagesIHKvexicaNo ratings yet
- MARET 2013: Minggu Senin Selasa Rabu Kamis Jumat SabtuDocument4 pagesMARET 2013: Minggu Senin Selasa Rabu Kamis Jumat SabtuvexicaNo ratings yet
- Ms. WordDocument1 pageMs. WordvexicaNo ratings yet
- 22 - Disease Biology PDFDocument28 pages22 - Disease Biology PDFashutosh samalNo ratings yet
- Peterson 2018Document21 pagesPeterson 2018Simal KhanNo ratings yet
- ChemotherapyDocument11 pagesChemotherapyNedaAbdullahNo ratings yet
- Antibiotic in OmfsDocument47 pagesAntibiotic in OmfsRajat GuptaNo ratings yet
- Preps 4-61Document57 pagesPreps 4-61fianaNo ratings yet
- Natural Products as Sources of Pharmaceutical LeadsDocument15 pagesNatural Products as Sources of Pharmaceutical LeadsQudsia RehmanNo ratings yet
- Everything You Need to Know About SyphilisDocument8 pagesEverything You Need to Know About SyphilisGandri Ali MasumNo ratings yet
- USMLE Practice Questions on BacteriologyDocument67 pagesUSMLE Practice Questions on BacteriologyKiran KrupaNo ratings yet
- Cephalothin SodiumDocument6 pagesCephalothin SodiumBeans JohnNo ratings yet
- Fournier Gangrene Causes and AnatomyDocument16 pagesFournier Gangrene Causes and AnatomyAmirah Dahalan100% (1)
- Drug StudyDocument10 pagesDrug StudybaniniycsebNo ratings yet
- Piperacillin MHRADocument46 pagesPiperacillin MHRAVaradha Raja PerumalNo ratings yet
- Antibiotics: Classification and ExamplesDocument39 pagesAntibiotics: Classification and ExamplesV G Viju KumarNo ratings yet
- An Tibi OtikDocument8 pagesAn Tibi OtikMuthi MelatiaraNo ratings yet
- CC 202014 20us6r 20ri 20se 20ia1Document8 pagesCC 202014 20us6r 20ri 20se 20ia1api-292667474No ratings yet
- Five chemistry inventions that enabled the modern worldDocument29 pagesFive chemistry inventions that enabled the modern worldzaimNo ratings yet
- Anh Chuyên NghànhDocument12 pagesAnh Chuyên Nghànhngoc anh doanNo ratings yet
- Control of Microorganisms Unit 7Document67 pagesControl of Microorganisms Unit 7Naseca100% (1)
- 5) General BacteriologyDocument86 pages5) General BacteriologyIanBiagtanNo ratings yet
- Drug Study (Pedia)Document7 pagesDrug Study (Pedia)Caurrine Monsalud100% (1)
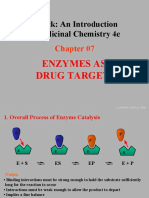
- Patrick: An Introduction To Medicinal Chemistry 4e: Enzymes As Drug TargetsDocument43 pagesPatrick: An Introduction To Medicinal Chemistry 4e: Enzymes As Drug TargetsVishaka KashyapNo ratings yet
- Acute GastritisDocument14 pagesAcute GastritisMenchie Vivas-AlotNo ratings yet
- 1 s2.0 S2667031322000355 MainDocument10 pages1 s2.0 S2667031322000355 MainSteffi NotaNo ratings yet
- Penicillins: Classification, Mechanism of Action & UsesDocument58 pagesPenicillins: Classification, Mechanism of Action & UsesSally PujaNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJanah PagayNo ratings yet
- UW Notes - 3 - MicrobiologyDocument45 pagesUW Notes - 3 - MicrobiologyKimberly KanemitsuNo ratings yet
- ? PHARMA 3. Anti InfectivesDocument130 pages? PHARMA 3. Anti InfectivesMiguel Luis NavarreteNo ratings yet
- Updated guidelines for initial antibiotic treatment of community-acquired pneumoniaDocument30 pagesUpdated guidelines for initial antibiotic treatment of community-acquired pneumoniachronos6534No ratings yet
- Biotechnology in Medical Industry: Prepared by Hilal Marangoz Sevgi DoğanDocument79 pagesBiotechnology in Medical Industry: Prepared by Hilal Marangoz Sevgi DoğanHilal MarangozNo ratings yet
- Extended Spectrum Penicillins and Their UsesDocument80 pagesExtended Spectrum Penicillins and Their UsesSunanda mohanNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)