You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Biological Warfare Agents - AgronDocument129 pagesBiological Warfare Agents - AgronMARK ARQUE LACANARIANo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Chapter 1Document27 pagesChapter 1CharleneKronstedtNo ratings yet
- Chapter 1 QuantitativeDocument39 pagesChapter 1 QuantitativeCharleneKronstedt100% (1)
- The Black Death EssayDocument10 pagesThe Black Death EssayDelciateNo ratings yet
- Super Sonic Logos: The Power of Audio BrandingDocument30 pagesSuper Sonic Logos: The Power of Audio BrandingCharleneKronstedtNo ratings yet
- Managing For Accountability: A Business Leader's ToolboxDocument32 pagesManaging For Accountability: A Business Leader's ToolboxCharleneKronstedt100% (1)
- Chapter 1Document46 pagesChapter 1CharleneKronstedtNo ratings yet
- Gram Negative Rods GuideDocument8 pagesGram Negative Rods GuideRuel Maddawin100% (1)
- Bioterrorism and Intelligence PDFDocument11 pagesBioterrorism and Intelligence PDFIbs Júnior100% (1)
- Handbook of Sustainable Development: Strategies For Organizational SustainabilityDocument57 pagesHandbook of Sustainable Development: Strategies For Organizational SustainabilityCharleneKronstedtNo ratings yet
- Rain Maker Pro: A Manager's Guide For Training SalespeopleDocument30 pagesRain Maker Pro: A Manager's Guide For Training SalespeopleCharleneKronstedtNo ratings yet
- Best Boss!Document40 pagesBest Boss!CharleneKronstedtNo ratings yet
- Chapter 1 PDFDocument30 pagesChapter 1 PDFCharleneKronstedtNo ratings yet
- Business Sustainability: Investor, Board, and Management PerspectiveDocument34 pagesBusiness Sustainability: Investor, Board, and Management PerspectiveCharleneKronstedtNo ratings yet
- Chapter 1 StrategicDocument36 pagesChapter 1 StrategicCharleneKronstedtNo ratings yet
- Understanding The Indian Economy From The Post-Reforms of 1991, Volume III: Indian AgricultureDocument33 pagesUnderstanding The Indian Economy From The Post-Reforms of 1991, Volume III: Indian AgricultureCharleneKronstedtNo ratings yet
- Ask The Right Questions Get The Right Job: Navigating The Job Interview To Take Control of Your CareerDocument44 pagesAsk The Right Questions Get The Right Job: Navigating The Job Interview To Take Control of Your CareerCharleneKronstedtNo ratings yet
- Branding & AIDocument46 pagesBranding & AICharleneKronstedtNo ratings yet
- Corporate Sustainability: Shareholder Primacy Versus Stakeholder PrimacyDocument28 pagesCorporate Sustainability: Shareholder Primacy Versus Stakeholder PrimacyCharleneKronstedtNo ratings yet
- Chapter 1 Strategic PDFDocument36 pagesChapter 1 Strategic PDFCharleneKronstedtNo ratings yet
- Chapter 1 Strategic PDFDocument36 pagesChapter 1 Strategic PDFCharleneKronstedtNo ratings yet
- Chapter 1Document35 pagesChapter 1CharleneKronstedtNo ratings yet
- Chapter 1Document63 pagesChapter 1CharleneKronstedt100% (1)
- Chapter 1Document41 pagesChapter 1CharleneKronstedtNo ratings yet
- Chapter 1Document63 pagesChapter 1CharleneKronstedt100% (1)
- Chapter 1Document27 pagesChapter 1CharleneKronstedtNo ratings yet
- Chapter 1Document26 pagesChapter 1CharleneKronstedtNo ratings yet
- Chapter 1Document40 pagesChapter 1CharleneKronstedtNo ratings yet
- Diseases That Are Preventable by VaccinationDocument33 pagesDiseases That Are Preventable by VaccinationCharleneKronstedt100% (1)
- Chapter 1Document33 pagesChapter 1CharleneKronstedtNo ratings yet
- Miller - Liberatore - Chapter 1Document27 pagesMiller - Liberatore - Chapter 1CharleneKronstedtNo ratings yet
- Chapter 1Document40 pagesChapter 1CharleneKronstedtNo ratings yet
- Friedman - Chapter 1Document21 pagesFriedman - Chapter 1CharleneKronstedt0% (1)
- Chapter 1Document25 pagesChapter 1CharleneKronstedtNo ratings yet
- COMPILATION ON MOOSHIKA VISHA .R. Guna SoundariDocument28 pagesCOMPILATION ON MOOSHIKA VISHA .R. Guna SoundariGuna SoundariNo ratings yet
- المختص في الحشرات -Synopsis of Medical EntomologyاDocument63 pagesالمختص في الحشرات -Synopsis of Medical EntomologyاDrMohamedBenrashedNo ratings yet
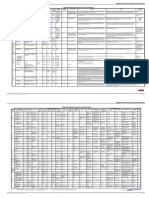
- Biological and Chemical Agent CharacteristicsDocument2 pagesBiological and Chemical Agent Characteristicsyiaili1234100% (1)
- Middle Age/ Medieval Period: Kent W. DepaysoDocument30 pagesMiddle Age/ Medieval Period: Kent W. DepaysoCindy MaslagNo ratings yet
- Medicine and Power in Tunisia, 1780-1900-Cambridge University Press (1983) PDFDocument161 pagesMedicine and Power in Tunisia, 1780-1900-Cambridge University Press (1983) PDFKam BouNo ratings yet
- 29 Theodor Dimitrov3Toward The Impact of The Justinianic Plague (541-750) On The Demographic Structure of The Byzantine EmpireDocument14 pages29 Theodor Dimitrov3Toward The Impact of The Justinianic Plague (541-750) On The Demographic Structure of The Byzantine EmpiretheodorrNo ratings yet
- Summary of Bacterial Infections of The SkinDocument11 pagesSummary of Bacterial Infections of The SkinYna Joy B. LigatNo ratings yet
- Black Death The Causes and Effects of A PandemicDocument13 pagesBlack Death The Causes and Effects of A PandemicThanh Cong NguyenNo ratings yet
- Background Medical CountermeasuresDocument7 pagesBackground Medical Countermeasuresapi-246003035No ratings yet
- Case Definitions For Infectious Diseases in Malaysia 2nd Edition Jan 2006Document110 pagesCase Definitions For Infectious Diseases in Malaysia 2nd Edition Jan 2006Veronica Vivi67% (3)
- Controle Global É TestadoDocument11 pagesControle Global É TestadoDavidson Leandro Silva dos SantosNo ratings yet
- Njhs Essay ExampleDocument6 pagesNjhs Essay Examplextnzpacaf100% (2)
- Case Study of Black Death: Our Lady of Fatima UniversityDocument7 pagesCase Study of Black Death: Our Lady of Fatima UniversityJanna PimentelNo ratings yet
- Micro Bio Disease ListDocument168 pagesMicro Bio Disease Listspiff spacemanNo ratings yet
- Photo EssayDocument13 pagesPhoto Essayapi-314854412No ratings yet
- Botany AssignmentDocument21 pagesBotany Assignmentabdul hadiNo ratings yet
- PLAGUE in Ecuador. PesteDocument11 pagesPLAGUE in Ecuador. PesteConsuelo QuispeNo ratings yet
- Black Death Encore FA10Document26 pagesBlack Death Encore FA10Chandni JeswaniNo ratings yet
- PLAGUE: Medical Management and Countermeasure Development.Document52 pagesPLAGUE: Medical Management and Countermeasure Development.Dmitri PopovNo ratings yet
- Plague Presentation FinalDocument41 pagesPlague Presentation FinalMazlan MansorNo ratings yet
- 7 Case Definitions of Infectious Disease in MalaysiaDocument110 pages7 Case Definitions of Infectious Disease in MalaysiaICNo ratings yet
- PlagueDocument20 pagesPlagueHemanth G.No ratings yet
- PlagueDocument31 pagesPlaguelulondon1No ratings yet
- Bubonic PlagueDocument408 pagesBubonic PlagueCotabus100% (1)
- Byzantine Studies Conference, 1976Document40 pagesByzantine Studies Conference, 1976ElisabetaNegrăuNo ratings yet
- Provision of A Safe EnvironmentDocument19 pagesProvision of A Safe EnvironmentKristian Jane de JesusNo ratings yet