You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Prenatal ScreeningDocument26 pagesPrenatal ScreeningbbyesNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Tocolytics in PretermDocument13 pagesTocolytics in PretermbbyesNo ratings yet
- Early Pregnancy ComplciationsDocument43 pagesEarly Pregnancy ComplciationsbbyesNo ratings yet
- Substance Abuse in PregnancyDocument151 pagesSubstance Abuse in PregnancybbyesNo ratings yet
- Pead 1 - NeonatologyDocument21 pagesPead 1 - NeonatologybbyesNo ratings yet
- Surgical - Information GuideDocument2 pagesSurgical - Information GuidebbyesNo ratings yet
- BASIC Course Gosford June 2021Document3 pagesBASIC Course Gosford June 2021bbyesNo ratings yet
- Guideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisDocument18 pagesGuideline: Maternity - Maternal Group B Streptococcus (GBS) and Minimisation of Neonatal Early-Onset GBS SepsisbbyesNo ratings yet
- SSIC Program of Delivery: Should Be Completed (Week) Date Orientation Evening and Entrance ExamDocument4 pagesSSIC Program of Delivery: Should Be Completed (Week) Date Orientation Evening and Entrance ExambbyesNo ratings yet
- Position Description ENTDocument3 pagesPosition Description ENTbbyesNo ratings yet
- Infections in PregnancyDocument11 pagesInfections in PregnancybbyesNo ratings yet
- Advanced Life Support AssessmentDocument1 pageAdvanced Life Support AssessmentbbyesNo ratings yet
- HMO Surgical PositionDocument4 pagesHMO Surgical PositionbbyesNo ratings yet
- RHDDocument130 pagesRHDDeepu RajendranNo ratings yet
- Ischkwa DiagramDocument1 pageIschkwa DiagrambbyesNo ratings yet
- Training Manual 2020Document53 pagesTraining Manual 2020bbyesNo ratings yet
- Atrial Fibrillation Managing Acute Atrial FibrillationDocument8 pagesAtrial Fibrillation Managing Acute Atrial FibrillationbbyesNo ratings yet
- Right VATS Pleural BiopsyDocument4 pagesRight VATS Pleural BiopsybbyesNo ratings yet
- C SpineDocument44 pagesC SpinebbyesNo ratings yet
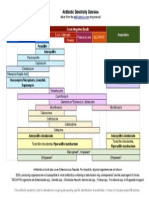
- Antibiotic Sensitivity Overview: Gram Positive Cocci Gram Negative Bacilli AnaerobesDocument1 pageAntibiotic Sensitivity Overview: Gram Positive Cocci Gram Negative Bacilli AnaerobesGuillermo Damian RodriguezNo ratings yet
- Shoulder PainDocument5 pagesShoulder PainbbyesNo ratings yet
- Upper GI BleedDocument8 pagesUpper GI BleedbbyesNo ratings yet
- Organisation Chart - TraineeDocument1 pageOrganisation Chart - TraineebbyesNo ratings yet
- ECGs - UpdatedDocument26 pagesECGs - UpdatedbbyesNo ratings yet
- Pump Manual TextDocument17 pagesPump Manual TextbbyesNo ratings yet
- Weekly SDS Topics: Week 3Document1 pageWeekly SDS Topics: Week 3bbyesNo ratings yet
- Prof PracDocument3 pagesProf PracbbyesNo ratings yet
- Main Presentations of Sexually Transmitted Infections in MenDocument3 pagesMain Presentations of Sexually Transmitted Infections in MenbbyesNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Therapeutic Management of Clinical Mastitis in Goat: A Case StudyDocument5 pagesTherapeutic Management of Clinical Mastitis in Goat: A Case StudyIJAR JOURNALNo ratings yet
- Module Answers 1 60 MCN 2Document151 pagesModule Answers 1 60 MCN 2bekbekk cabahug100% (6)
- Nursing Care of Patients With Digestive & Gastrointestinal DisordersDocument29 pagesNursing Care of Patients With Digestive & Gastrointestinal DisordersjoreyneeNo ratings yet
- ICON 2016 Febrile Neutropenia GuidelinesDocument34 pagesICON 2016 Febrile Neutropenia GuidelinesTor Ja100% (1)
- Dulcolax Stool Softener Supp (Docusate Sodium)Document2 pagesDulcolax Stool Softener Supp (Docusate Sodium)ENo ratings yet
- Schedule of Charges - April 2015Document69 pagesSchedule of Charges - April 2015Chocolete HeartNo ratings yet
- Maternal and Child HealthDocument60 pagesMaternal and Child HealthStar AcademyNo ratings yet
- Exercise Tolerance TestDocument15 pagesExercise Tolerance TestahmedNo ratings yet
- High Volume HDF - Scientific Brochure - EN - 01oct2018 - Approved - Original - 112Document2 pagesHigh Volume HDF - Scientific Brochure - EN - 01oct2018 - Approved - Original - 112HARUMUKIZA Jean DomitienNo ratings yet
- Endocrine Glands - 1st - ChapterDocument12 pagesEndocrine Glands - 1st - Chaptervarun kumarNo ratings yet
- PHARM 315: Cheza May Baldado BS Pharm IIIDocument12 pagesPHARM 315: Cheza May Baldado BS Pharm IIIKathleen B BaldadoNo ratings yet
- Clinical Manual - Part 2 - Drug Infusion Guidelines Revised - July 2015 - V7.11Document58 pagesClinical Manual - Part 2 - Drug Infusion Guidelines Revised - July 2015 - V7.11Jayaprakash KuppusamyNo ratings yet
- Che 222 Population Dynamics and Family PlanningDocument53 pagesChe 222 Population Dynamics and Family PlanningArum Comrade100% (1)
- YS Curodont Sell Sheet - 8.5x11 - FINAL 1Document1 pageYS Curodont Sell Sheet - 8.5x11 - FINAL 1lucian hahaianuNo ratings yet
- Rubber Band Ligation: of HaemorrhoidsDocument1 pageRubber Band Ligation: of HaemorrhoidsdbedadaNo ratings yet
- Homeopathic ImmunizationDocument53 pagesHomeopathic Immunizationalex100% (2)
- Thyroid Eye Disease Diagnosis and TreatmentDocument486 pagesThyroid Eye Disease Diagnosis and TreatmentUnsmil UnguNo ratings yet
- FCEM (SA) Part II Past Papers - 2012 Sept 22-1-2014Document7 pagesFCEM (SA) Part II Past Papers - 2012 Sept 22-1-2014matentenNo ratings yet
- Konsep Wound ManajemenDocument24 pagesKonsep Wound ManajemenNiken DewiNo ratings yet
- Opioid Adjuvant in NeuraxialDocument10 pagesOpioid Adjuvant in NeuraxialiswanlatifNo ratings yet
- Carcinocine in PaediatricsDocument5 pagesCarcinocine in Paediatricssimiliadoc100% (1)
- Ready Reckoner For Class Room 08-01-2020Document70 pagesReady Reckoner For Class Room 08-01-2020yoNo ratings yet
- T2DM PracticalGuide 20190718 FA Ebook2Document80 pagesT2DM PracticalGuide 20190718 FA Ebook2Nokoline HuNo ratings yet
- Managing Tumor Lysis Syndrome.2Document4 pagesManaging Tumor Lysis Syndrome.2Caballero X CaballeroNo ratings yet
- A Simple Approach To Shared Decision Making in Cancer ScreeningDocument6 pagesA Simple Approach To Shared Decision Making in Cancer ScreeningariskaNo ratings yet
- Dental Management of The Patient With HIVAIDS 2002Document6 pagesDental Management of The Patient With HIVAIDS 2002drkameshNo ratings yet
- Complete Medical TermsDocument32 pagesComplete Medical TermsSharifa Darayan100% (1)
- Drug StudyDocument7 pagesDrug StudyArnel MacabalitaoNo ratings yet
- Test Bank For Pharmacology and The Nursing Process 9th by LilleyDocument6 pagesTest Bank For Pharmacology and The Nursing Process 9th by LilleyJames Philhower100% (30)
- Lesson 3. Physiological Basis of BehaviorDocument46 pagesLesson 3. Physiological Basis of BehaviorMary Ann DimayugaNo ratings yet