You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Potenciometro 15KDocument8 pagesPotenciometro 15Kra101208No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Eurotech IoT Gateway Reliagate 10 12 ManualDocument88 pagesEurotech IoT Gateway Reliagate 10 12 Manualfelix olguinNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Music GcseDocument45 pagesMusic GcseAimee DohertyNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- DC Machines Chapter SummaryDocument14 pagesDC Machines Chapter SummaryMajad RazakNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
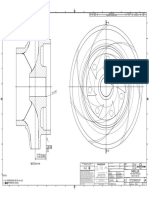
- Impeller: REV Rev by Description PCN / Ecn Date CHK'D A JMM Released For Production N/A 18/11/2019 PDLDocument1 pageImpeller: REV Rev by Description PCN / Ecn Date CHK'D A JMM Released For Production N/A 18/11/2019 PDLSenthilkumar RamalingamNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Astm D5501Document3 pagesAstm D5501mhmdgalalNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Displaymax JR 1500 SpecsDocument1 pageDisplaymax JR 1500 SpecsFRANCISCONo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Solvent based printing inks applicationsDocument34 pagesSolvent based printing inks applicationsAmna liaquatNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Linear Thermal Expansion of Solid Materials With A Vitreous Silica DilatometerDocument7 pagesLinear Thermal Expansion of Solid Materials With A Vitreous Silica Dilatometerluis_may22No ratings yet
- HowTo Work With CR 90Document87 pagesHowTo Work With CR 90WagBezerraNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hawking-Brief History of TimeDocument336 pagesHawking-Brief History of TimeAlbert Kristian0% (1)
- 11+ Entrance Examination: Specimen PaperDocument8 pages11+ Entrance Examination: Specimen PaperNayem Hossain HemuNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- QT140 500 KG Per Hr. Fish Feed Pelleting PlantDocument11 pagesQT140 500 KG Per Hr. Fish Feed Pelleting PlantShekhar MitraNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 1.11 CHEM FINAL Chapter 11 Sulfuric AcidDocument21 pages1.11 CHEM FINAL Chapter 11 Sulfuric AcidSudhanshuNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Wartsila CPP PaperDocument4 pagesWartsila CPP Papergatheringforgardner9550No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- ISO 8243 2013 Cigarettes - SamplingDocument18 pagesISO 8243 2013 Cigarettes - SamplingEko YuliantoNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- A Design and Analysis of A Morphing Hyper-Elliptic Cambered Span (HECS) WingDocument10 pagesA Design and Analysis of A Morphing Hyper-Elliptic Cambered Span (HECS) WingJEORJENo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Data AnalysisDocument7 pagesData AnalysisAndrea MejiaNo ratings yet
- Training Matrix For TM IDocument14 pagesTraining Matrix For TM IApril NavaretteNo ratings yet
- 000 200 1210 Guidelines For Minimum Deliverables 3 November 2011Document22 pages000 200 1210 Guidelines For Minimum Deliverables 3 November 2011Raul Bautista100% (1)
- Example 1 LS Dyna - Bullet Model SimulationDocument6 pagesExample 1 LS Dyna - Bullet Model Simulationsunil_vrvNo ratings yet
- Dynamic Modeling of GE 1.5 andDocument31 pagesDynamic Modeling of GE 1.5 andErtuğrul ÇamNo ratings yet
- HI-8592, HI-8593, HI-8594: Single-Rail ARINC 429 Differential Line DriverDocument14 pagesHI-8592, HI-8593, HI-8594: Single-Rail ARINC 429 Differential Line DriversameeppaiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- OracleDocument23 pagesOracleriza arifNo ratings yet
- 1/2" Cellflex Superflexible Foam-Dielectric Coaxial Cable: SCF12-50JDocument2 pages1/2" Cellflex Superflexible Foam-Dielectric Coaxial Cable: SCF12-50JpeguigonsoNo ratings yet
- ASP Flashcards - QuizletDocument36 pagesASP Flashcards - QuizletRehman MuzaffarNo ratings yet
- PTP - Level MethodsDocument23 pagesPTP - Level Methodssasikiran mNo ratings yet
- Smart Dustbin using ArduinoDocument22 pagesSmart Dustbin using ArduinoEr Dinesh TambeNo ratings yet
- Determination of Voltage DropDocument6 pagesDetermination of Voltage DropFahmi CumiNo ratings yet
- Analisis Pengaruh Profitabilitas, Strategi Diversifikasi, Dan Good Corporate Governance Terhadap Nilai PerusahaanDocument16 pagesAnalisis Pengaruh Profitabilitas, Strategi Diversifikasi, Dan Good Corporate Governance Terhadap Nilai PerusahaanEra ZsannabelaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)