You might also like
- Comparison of Repeatability Between Intraoral Digital Scanner and Extraoral Digital Scanner An Invitro Study.Document7 pagesComparison of Repeatability Between Intraoral Digital Scanner and Extraoral Digital Scanner An Invitro Study.Alex BurdeNo ratings yet
- Digital WorkflowsDocument14 pagesDigital Workflowsmoji_puiNo ratings yet
- Cad CamDocument5 pagesCad CamNajeeb UllahNo ratings yet
- Accuracy of Implant Placement With Computer-Guided SurgeryDocument15 pagesAccuracy of Implant Placement With Computer-Guided SurgerydentureNo ratings yet
- CEREC Basic Information 3.8Document134 pagesCEREC Basic Information 3.8Ivan Georgiev100% (1)
- Erec Eneers: How, When & WhyDocument42 pagesErec Eneers: How, When & WhyAshraf SawyNo ratings yet
- Thecurrentstateof Chairsidedigitaldentistry Andmaterials: Markus B. Blatz,, Julian ConejoDocument23 pagesThecurrentstateof Chairsidedigitaldentistry Andmaterials: Markus B. Blatz,, Julian ConejoMichelle VargasNo ratings yet
- Cerec 3d Preparation Guidelines en PDFDocument10 pagesCerec 3d Preparation Guidelines en PDFMarian Si Teofana HasnaNo ratings yet
- Introduction To Guided Implant SurgeryDocument9 pagesIntroduction To Guided Implant SurgeryVioleta Botnari100% (1)
- Neodent Guided Kit PDFDocument24 pagesNeodent Guided Kit PDFBehdad JavdanNo ratings yet
- Exoplan.3.1.user Manual Surgical Guide ENDocument229 pagesExoplan.3.1.user Manual Surgical Guide ENElena RezaeiNo ratings yet
- Cad/Cam Complete Dentures: A Review of Two Commercial: Fabrication SystemsDocument10 pagesCad/Cam Complete Dentures: A Review of Two Commercial: Fabrication SystemsEugenStanciuNo ratings yet
- IDD CAD CAM Intraoral Scanner Reviews IDS 2019 May UpdateDocument30 pagesIDD CAD CAM Intraoral Scanner Reviews IDS 2019 May UpdateAndrew VillanuevaNo ratings yet
- CAD/CAM Dentistry and Chairside Digital Impression Making: 4 CE CreditsDocument11 pagesCAD/CAM Dentistry and Chairside Digital Impression Making: 4 CE CreditsShraddha AgarwalNo ratings yet
- MoGuFi 2007 GB 1Document1 pageMoGuFi 2007 GB 1Iulian GheorgheNo ratings yet
- Cad CamDocument5 pagesCad CamsauriuaNo ratings yet
- SKY Implant System - Technical DataDocument40 pagesSKY Implant System - Technical DataAda BaloNo ratings yet
- Guided Surgery Technique Associated To Morse Taper Implants With A Hexagonal Internal IndexDocument16 pagesGuided Surgery Technique Associated To Morse Taper Implants With A Hexagonal Internal IndexLalaNo ratings yet
- Kodak 3D 電腦斷層系統Document28 pagesKodak 3D 電腦斷層系統fomed_twNo ratings yet
- Digital Impressions - A Review of Latest PDFDocument5 pagesDigital Impressions - A Review of Latest PDFSonali KinikarNo ratings yet
- LAB Brochure Inlab Cad Software Design en PDFDocument13 pagesLAB Brochure Inlab Cad Software Design en PDFJuan Carlos RomeroNo ratings yet
- Digital Impressions A New Era in ProsthodonticsDocument3 pagesDigital Impressions A New Era in Prosthodonticsaziz2007No ratings yet
- Asymmetric Extractions in Orthodontics PDFDocument6 pagesAsymmetric Extractions in Orthodontics PDFOsama MohamedNo ratings yet
- Straumann® Guided Surgery System InstrumentsDocument48 pagesStraumann® Guided Surgery System InstrumentsSupaluk Mod ChuencheepNo ratings yet
- Bopt PanizDocument9 pagesBopt PanizIvan CarreraNo ratings yet
- Seminar TopicsDocument1 pageSeminar TopicsDadi SindhuNo ratings yet
- Prosthetic Dentistry 1916Document1,248 pagesProsthetic Dentistry 1916lotusfrog100% (1)
- Narrow Diameter Dental Implant: Reporter ModeratorDocument71 pagesNarrow Diameter Dental Implant: Reporter ModeratorkangleisNo ratings yet
- Metallurgical and Interfacial Characterization of PFM Co-Cr Dental Alloys Fabricated Via Casting, Milling or Selective Laser MeltingDocument10 pagesMetallurgical and Interfacial Characterization of PFM Co-Cr Dental Alloys Fabricated Via Casting, Milling or Selective Laser MeltingCiubotaru Andrei-GabrielNo ratings yet
- SKY Implant System - Titanium - GBDocument40 pagesSKY Implant System - Titanium - GBCipy XyzxNo ratings yet
- 3d Printing in Fixed ProsthodonticsDocument5 pages3d Printing in Fixed ProsthodonticsCherifNo ratings yet
- 3shape Clear Aligner Studio End User HandbookDocument9 pages3shape Clear Aligner Studio End User HandbookFinhasNo ratings yet
- Copy Dentures: Presenter DR Obiero Moderator DR Omondi 2/3/2021Document58 pagesCopy Dentures: Presenter DR Obiero Moderator DR Omondi 2/3/2021elishaNo ratings yet
- Endo LaseDocument5 pagesEndo LaseAlex PaunNo ratings yet
- Management of Peri-Implant Mucositis and Peri-Implantitis PDFDocument19 pagesManagement of Peri-Implant Mucositis and Peri-Implantitis PDFgirl33No ratings yet
- Installation Nt-IQ Library 3shapeDocument5 pagesInstallation Nt-IQ Library 3shapeThaer Saad Al DeenNo ratings yet
- Iti Implant Course 2018 PDFDocument5 pagesIti Implant Course 2018 PDFShyam K MaharjanNo ratings yet
- Digital Technologies in DentistryDocument96 pagesDigital Technologies in Dentistryابو سارة100% (1)
- Goldstein Re Esthetics in DentistryDocument3 pagesGoldstein Re Esthetics in DentistryMichaelNo ratings yet
- Digitalalisation in Dentistry PDFDocument19 pagesDigitalalisation in Dentistry PDF林元敏No ratings yet
- Finishing and Detailing in OrthodonticsDocument6 pagesFinishing and Detailing in OrthodonticsRohini TondaNo ratings yet
- Bicon Short Implant 1Document6 pagesBicon Short Implant 1Bicon Implant InaNo ratings yet
- Emax CAD Step Cerec-E - 627931Document2 pagesEmax CAD Step Cerec-E - 627931Leo JamesNo ratings yet
- A Modification of The Altered Cast TechniqueDocument2 pagesA Modification of The Altered Cast TechniqueChirag Gorasiya100% (1)
- Sling and Tag Suturing Technique For Coronally Advanced FlapDocument7 pagesSling and Tag Suturing Technique For Coronally Advanced FlapFerdinan Pasaribu0% (1)
- Bonnick - 2011 - Dental Clinics of North America PDFDocument14 pagesBonnick - 2011 - Dental Clinics of North America PDFKranti PrajapatiNo ratings yet
- Digital Versus Conventional Impressions For Fixed Prosthodontics: A Systematic Review and Meta-AnalysisDocument19 pagesDigital Versus Conventional Impressions For Fixed Prosthodontics: A Systematic Review and Meta-AnalysisÁł ÃăNo ratings yet
- Maestro 3d Ortho Studio User Manual enDocument49 pagesMaestro 3d Ortho Studio User Manual enNamBui100% (1)
- 3 D PrintingDocument4 pages3 D PrintingProsthodontics DeptNo ratings yet
- JC 12 Clinical Efficacy of Methods For Bonding To ZirconiaDocument37 pagesJC 12 Clinical Efficacy of Methods For Bonding To ZirconiaMrinmayee ThakurNo ratings yet
- Comparison of Tooth Shade Matching Using Visual and Digital Camera MethodsDocument5 pagesComparison of Tooth Shade Matching Using Visual and Digital Camera Methodsjanicesusanto2000No ratings yet
- Cobalt-Chromium Alloys in Dentistry An Evaluation of Metal Ion ReleaseDocument7 pagesCobalt-Chromium Alloys in Dentistry An Evaluation of Metal Ion ReleaseFrank LucariniNo ratings yet
- Rotary Systems: An Insight: Manmohan R Soni, Swaroop Hegde, Sylvia Mathew, K S MadhuDocument6 pagesRotary Systems: An Insight: Manmohan R Soni, Swaroop Hegde, Sylvia Mathew, K S MadhuIulia Florina SimaNo ratings yet
- Vsip - Info - Anterior Wax Up PDF Free PDFDocument3 pagesVsip - Info - Anterior Wax Up PDF Free PDFMekideche dental officeNo ratings yet
- Periodontal Microsurgery: Home Mcq's Discussions ContactDocument8 pagesPeriodontal Microsurgery: Home Mcq's Discussions Contactdileep9002392No ratings yet
- Provisional MaterialsDocument4 pagesProvisional Materialsveloso.rossana100% (1)
- Titanium in Dentistry Historical Development State of The Art PDFDocument7 pagesTitanium in Dentistry Historical Development State of The Art PDFPabloNo ratings yet
- Retention of Maxillofacial Prosthesis PDFDocument6 pagesRetention of Maxillofacial Prosthesis PDFBismita PradhanNo ratings yet
- Sicat Surgical Guide Manual PDFDocument56 pagesSicat Surgical Guide Manual PDFvashishtanatomyNo ratings yet
- Evaluation Of-Titanium-Alloy-Fabricated-Using-Electron-Beam-Melting-And-Traditional-Casting-TechniqueDocument7 pagesEvaluation Of-Titanium-Alloy-Fabricated-Using-Electron-Beam-Melting-And-Traditional-Casting-TechniqueAlex BurdeNo ratings yet
- PolyJet Case Study - Albensi Dental Lab Jewel in The Crown ENDocument2 pagesPolyJet Case Study - Albensi Dental Lab Jewel in The Crown ENAlex BurdeNo ratings yet
- Trueness Analysis of Zirconia Crowns Fabricated With 3d PrintingDocument7 pagesTrueness Analysis of Zirconia Crowns Fabricated With 3d PrintingAlex BurdeNo ratings yet
- A 3D Printing Replication Technique For Fabricating Digital DenturesDocument6 pagesA 3D Printing Replication Technique For Fabricating Digital DenturesAlex BurdeNo ratings yet
- PolyJet Case Study - Allure Dental Studio Gold Tooth ENDocument2 pagesPolyJet Case Study - Allure Dental Studio Gold Tooth ENAlex BurdeNo ratings yet
- PolyJet Case Study - Dawood and Tanner EN A4 - 0818aDocument4 pagesPolyJet Case Study - Dawood and Tanner EN A4 - 0818aAlex BurdeNo ratings yet
- 3D Printing in Orthognathic SurgeryDocument12 pages3D Printing in Orthognathic SurgeryAlex BurdeNo ratings yet
- PolyJet Case Study - Biogenic Dental Corporation - Increased Capacity ENDocument3 pagesPolyJet Case Study - Biogenic Dental Corporation - Increased Capacity ENAlex BurdeNo ratings yet
- Accuracy of 3D Printed Models Created by Two Technologies of Printers With Different Designs of Model BaseDocument5 pagesAccuracy of 3D Printed Models Created by Two Technologies of Printers With Different Designs of Model BaseAlex BurdeNo ratings yet
- A 3D Printing Replication Technique For Fabricating Digital DenturesDocument6 pagesA 3D Printing Replication Technique For Fabricating Digital DenturesAlex BurdeNo ratings yet
- 3D Printing Trends 2020: Industry Highlights and Market TrendsDocument38 pages3D Printing Trends 2020: Industry Highlights and Market TrendsAlex BurdeNo ratings yet
- PolyJet Best Practice EN - MED625FLX Dental ApplicationsDocument4 pagesPolyJet Best Practice EN - MED625FLX Dental ApplicationsAlex BurdeNo ratings yet
- An Update On Applications of 3D Printing Technologies UsedDocument8 pagesAn Update On Applications of 3D Printing Technologies UsedAlex BurdeNo ratings yet
- Applications of 3D Printing On Craniofacial Bone Repair A Systematic ReviewDocument14 pagesApplications of 3D Printing On Craniofacial Bone Repair A Systematic ReviewAlex BurdeNo ratings yet
- Three-Dimensional Printing Biotechnology For The Regeneration of The Tooth and Tooth-Supporting TissuesDocument52 pagesThree-Dimensional Printing Biotechnology For The Regeneration of The Tooth and Tooth-Supporting TissuesJuan Pablo Pereira GarcíaNo ratings yet
- 3D - Printing - Dentistry-State of The ArtDocument11 pages3D - Printing - Dentistry-State of The ArtAlex BurdeNo ratings yet
- Additive Manufacturing Techniques in Prosthodontics Where Do We Currently Stand A Critical ReviewDocument11 pagesAdditive Manufacturing Techniques in Prosthodontics Where Do We Currently Stand A Critical ReviewAlex BurdeNo ratings yet
- 3d PrintingDocument9 pages3d PrintingbkprosthoNo ratings yet
- How Useful Is 3D Printing in Maxillofacial SurgeryDocument19 pagesHow Useful Is 3D Printing in Maxillofacial SurgeryAlex BurdeNo ratings yet
- 3D Printing in Orthognathic SurgeryDocument12 pages3D Printing in Orthognathic SurgeryAlex BurdeNo ratings yet
- QDT 2001 PDFDocument239 pagesQDT 2001 PDFAlex BurdeNo ratings yet
- Idea Dientes de ResinaDocument20 pagesIdea Dientes de ResinaCocodriloSacamuelasNo ratings yet
- 3D Printed Teeth For The Preclinical EducationDocument7 pages3D Printed Teeth For The Preclinical EducationAlex BurdeNo ratings yet
- Guidelines: The Crown and Bridge TechniqueDocument23 pagesGuidelines: The Crown and Bridge TechniqueAlex Burde100% (1)
- Translucency and Masking Properties of Two Ceramic Materials For Heat-Press TechnologyDocument6 pagesTranslucency and Masking Properties of Two Ceramic Materials For Heat-Press TechnologyAlex BurdeNo ratings yet
- Idea Dientes de ResinaDocument20 pagesIdea Dientes de ResinaCocodriloSacamuelasNo ratings yet
- Accuracy of Dies Captured by An Intraoral Digital ImpressionDocument4 pagesAccuracy of Dies Captured by An Intraoral Digital ImpressionAlex BurdeNo ratings yet
- Direct Mechanical Data Acquisition of Dental Impressions For The Manufacturing of CAD-CAM RestorationsDocument6 pagesDirect Mechanical Data Acquisition of Dental Impressions For The Manufacturing of CAD-CAM RestorationsAlex BurdeNo ratings yet
- PM9 Working-Instructions 09Document48 pagesPM9 Working-Instructions 09Alex BurdeNo ratings yet
- Comparing Additive Manufacturing Technologies For Customised Wrist SplintsDocument27 pagesComparing Additive Manufacturing Technologies For Customised Wrist SplintsAlex BurdeNo ratings yet
- Java Inheritance PDFDocument7 pagesJava Inheritance PDFMallikarjun AradhyaNo ratings yet
- Relief Valve From HysysDocument8 pagesRelief Valve From Hysysarmin100% (1)
- Inverse of A Matrix Using Elementary Row Operations (Gauss-Jordan)Document5 pagesInverse of A Matrix Using Elementary Row Operations (Gauss-Jordan)Brian LeeNo ratings yet
- Toaz - Info Tutor Hack Via Termux PRDocument15 pagesToaz - Info Tutor Hack Via Termux PRPerwira Daing GuntaraNo ratings yet
- Firmware - WikipediaDocument3 pagesFirmware - WikipediaselbalNo ratings yet
- iDeskSDK 2020-04-12 LogDocument4 pagesiDeskSDK 2020-04-12 LogDoddyNo ratings yet
- MAT 105 SyllabusDocument2 pagesMAT 105 SyllabusAnkit SinghNo ratings yet
- InTouchOMI WhileOpenning LogSampleDocument40 pagesInTouchOMI WhileOpenning LogSampleStanislav NosirevNo ratings yet
- SP12 2y3 PC PP 993 007Document21 pagesSP12 2y3 PC PP 993 007Alex Ciupitu100% (1)
- Nexus 7k - Getting Started Examples - Part1 (Basics, VDC and VPC) - NetworkGeekStuffDocument26 pagesNexus 7k - Getting Started Examples - Part1 (Basics, VDC and VPC) - NetworkGeekStuffJean Jacques BelyNo ratings yet
- CSC Update LogDocument14 pagesCSC Update LogJuan Carlos Cáceres ReyesNo ratings yet
- Mohit Malik Web Developer PortfolioDocument21 pagesMohit Malik Web Developer PortfolioMohit MalikNo ratings yet
- Azure AD Mastery Training PlanDocument4 pagesAzure AD Mastery Training PlanArif Mohammed RangrezzNo ratings yet
- Anna University: Coimbatore M.C.A (Master of Computer Applications)Document9 pagesAnna University: Coimbatore M.C.A (Master of Computer Applications)rabin9999No ratings yet
- Anti Theft Control System IJERTCONV7IS08086Document6 pagesAnti Theft Control System IJERTCONV7IS08086Lloyd Christian BaringNo ratings yet
- Konica 7060 SolutionsDocument103 pagesKonica 7060 Solutionsjhall4363No ratings yet
- 2.1basic Assemblers FunctionsDocument15 pages2.1basic Assemblers FunctionsChanchal Rawat100% (1)
- Computer Network Thesis IdeasDocument8 pagesComputer Network Thesis Ideasdwtnpjyv100% (2)
- SD-WAN Comparison Chart: Cisco Velocloud Versa Silver PeakDocument6 pagesSD-WAN Comparison Chart: Cisco Velocloud Versa Silver PeaktotokNo ratings yet
- Philips 109b7Document90 pagesPhilips 109b7Charly HirschNo ratings yet
- By Coderipper / SND: Tools UsedDocument6 pagesBy Coderipper / SND: Tools UsedJhwazkdNo ratings yet
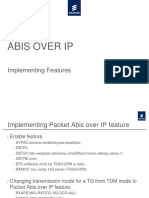
- ABIS OVER IP Implementing Features PDFDocument11 pagesABIS OVER IP Implementing Features PDFManish SharmaNo ratings yet
- Curriculum Vitae: Lakshmana Manikanta .VDocument3 pagesCurriculum Vitae: Lakshmana Manikanta .Vashok8164No ratings yet
- EE313 Lab 2Document6 pagesEE313 Lab 2Alvish NaiduNo ratings yet
- MeDocument2 pagesMeisaacamankwaaNo ratings yet
- ProxySG Required PortsDocument8 pagesProxySG Required PortsbooksmagicNo ratings yet
- Scheme ProgramingDocument43 pagesScheme Programingncs_19_cosmin424100% (1)
- Rakesh Yadav Sir Reasoning Book in HindiDocument161 pagesRakesh Yadav Sir Reasoning Book in HindiBalwinder SinghNo ratings yet
- FYBSC - AnimationDocument22 pagesFYBSC - AnimationSitanshu BhartiyaNo ratings yet