You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Sample Cover Letter Oil and GasDocument1 pageSample Cover Letter Oil and GasNadira Aqilah67% (3)
- SSTMCV Retail PowerDocument5 pagesSSTMCV Retail Powervipin.yadavNo ratings yet
- Kinetics of Acetone Hydrogenation For Synthesis of Isopropyl Alcohol Over Cu-Al Mixed Oxide CatalystsDocument9 pagesKinetics of Acetone Hydrogenation For Synthesis of Isopropyl Alcohol Over Cu-Al Mixed Oxide Catalysts李国俊No ratings yet
- Unit 06 Extra Grammar ExercisesDocument3 pagesUnit 06 Extra Grammar ExercisesLeo Muñoz43% (7)
- Matt Lewis Law Preparing & Presenting Compensability & Extent of Injury IssuesDocument11 pagesMatt Lewis Law Preparing & Presenting Compensability & Extent of Injury IssuesMatt Lewis LawNo ratings yet
- Matt Lewis Law Dallas Texas - Indemnity Dispute Resolution July 2009Document31 pagesMatt Lewis Law Dallas Texas - Indemnity Dispute Resolution July 2009Matt Lewis LawNo ratings yet
- Matt Lewis Law Dallas Texas - Indemnity Dispute Resolution July 2009Document31 pagesMatt Lewis Law Dallas Texas - Indemnity Dispute Resolution July 2009Matt Lewis LawNo ratings yet
- Matt Lewis Law - Libs Update 2015Document18 pagesMatt Lewis Law - Libs Update 2015Matt Lewis LawNo ratings yet
- Matt Lewis Law Dallas Texas - ODG - July 11, 2008Document31 pagesMatt Lewis Law Dallas Texas - ODG - July 11, 2008Matt Lewis LawNo ratings yet
- Costs-Concepts and ClassificationsDocument12 pagesCosts-Concepts and ClassificationsLune NoireNo ratings yet
- Opening Up The Prescriptive Authority PipelineDocument10 pagesOpening Up The Prescriptive Authority PipelineJohn GavazziNo ratings yet
- Chpter 06 QuizDocument3 pagesChpter 06 QuizGall AnonimNo ratings yet
- Wealth-Lab Developer 6.9 Performance: Strategy: Channel Breakout VT Dataset/Symbol: AALDocument1 pageWealth-Lab Developer 6.9 Performance: Strategy: Channel Breakout VT Dataset/Symbol: AALHamahid pourNo ratings yet
- 2008 Application FormDocument12 pages2008 Application FormVishal PonugotiNo ratings yet
- Modelo de NDA (English)Document2 pagesModelo de NDA (English)Jorge Partidas100% (3)
- S-S-, AXXX XXX 008 (BIA Sept. 15, 2017)Document7 pagesS-S-, AXXX XXX 008 (BIA Sept. 15, 2017)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- Motorola l6Document54 pagesMotorola l6Marcelo AriasNo ratings yet
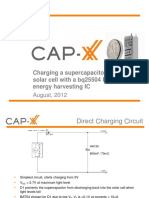
- 1208 CAP XX Charging A Supercapacitor From A Solar Cell PDFDocument12 pages1208 CAP XX Charging A Supercapacitor From A Solar Cell PDFmehralsmenschNo ratings yet
- 7 ways to improve energy efficiency of pumpsDocument1 page7 ways to improve energy efficiency of pumpsCharina Malolot VillalonNo ratings yet
- The Problem and Its SettingDocument36 pagesThe Problem and Its SettingRodel CamposoNo ratings yet
- Aesculap Qatar UniversityDocument3 pagesAesculap Qatar UniversityAl Quran AcademyNo ratings yet
- Ap22 FRQ World History ModernDocument13 pagesAp22 FRQ World History ModernDylan DanovNo ratings yet
- Speaking Telephone RoleplaysDocument2 pagesSpeaking Telephone RoleplaysremimiguelNo ratings yet
- Public Relations Proposal Template: Executive SummaryDocument3 pagesPublic Relations Proposal Template: Executive SummaryErmi SusilowatiNo ratings yet
- CJCuny Talmor PE TurnaroundsDocument18 pagesCJCuny Talmor PE TurnaroundsMayank Shankar SinghNo ratings yet
- Lecture 2 Leader-Centred PerspectivesDocument24 pagesLecture 2 Leader-Centred PerspectivesLIVINGSTONE CAESARNo ratings yet
- Marking SchemeDocument8 pagesMarking Schememohamed sajithNo ratings yet
- Draft SemestralWorK Aircraft2Document7 pagesDraft SemestralWorK Aircraft2Filip SkultetyNo ratings yet
- Foreign Direct Investment in Mongolia An Interactive Case Study (USAID, 2007)Document266 pagesForeign Direct Investment in Mongolia An Interactive Case Study (USAID, 2007)Oyuna Bat-OchirNo ratings yet
- Acuite-India Credit Risk Yearbook FinalDocument70 pagesAcuite-India Credit Risk Yearbook FinalDinesh RupaniNo ratings yet
- Office of The Controller of Examinations Anna University:: Chennai - 600 025Document4 pagesOffice of The Controller of Examinations Anna University:: Chennai - 600 025M.KARTHIKEYANNo ratings yet
- The Importance of Personal Protective Equipment in Pesticide App 2018Document4 pagesThe Importance of Personal Protective Equipment in Pesticide App 2018Anees MalikNo ratings yet
- Schoology App Login DirectionsDocument5 pagesSchoology App Login Directionsapi-234989244No ratings yet
- English Speech Save Our Earth Save Our RainforestDocument3 pagesEnglish Speech Save Our Earth Save Our RainforestYeremia Billy100% (1)
- MONETARY POLICY OBJECTIVES AND APPROACHESDocument2 pagesMONETARY POLICY OBJECTIVES AND APPROACHESMarielle Catiis100% (1)