You might also like
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument1 pageSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionAnonymous CKAborxxwNo ratings yet
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument8 pagesSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionNugroho TeguhNo ratings yet
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital Preparationgusti angri angalanNo ratings yet
- Posters For ClinicDocument80 pagesPosters For ClinicdenzkissaieNo ratings yet
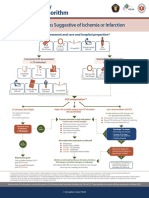
- Acute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or InfarctionDocument1 pageAcute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or Infarctionjohndoe1995No ratings yet
- Acut Coronary SyndromesDocument1 pageAcut Coronary SyndromesMuhittin Selçuk ÖzkanNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFJim Christian EllaserNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFNety Pandung SalembanNo ratings yet
- Paediatric Guidelines Croup 2020Document4 pagesPaediatric Guidelines Croup 2020nimraNo ratings yet
- ASTHMA - SemisDocument4 pagesASTHMA - SemisInday BertaNo ratings yet
- Acute Asthma - Care in The Emergency DepartmentDocument5 pagesAcute Asthma - Care in The Emergency DepartmentTanitNo ratings yet
- Ventolin DrugstudyDocument1 pageVentolin DrugstudyMsOrangeNo ratings yet
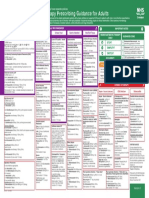
- Empirical Antimicrobial Therapy Prescribing Guidance For AdultsDocument1 pageEmpirical Antimicrobial Therapy Prescribing Guidance For AdultsPsychology TodayNo ratings yet
- Name of DrugDocument5 pagesName of DrugJoann BeriñoNo ratings yet
- Bronchospasm Child: PO 2-6 Y, 0.1-: 0.2 MG/KG T.I.D. (Max: 4 Mg/dose) 6-12 Y, 2 MG 3-4 Times/dDocument2 pagesBronchospasm Child: PO 2-6 Y, 0.1-: 0.2 MG/KG T.I.D. (Max: 4 Mg/dose) 6-12 Y, 2 MG 3-4 Times/dArnold De Guzman Jr.No ratings yet
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationIGOR SHEYNINNo ratings yet
- AsthmaDocument2 pagesAsthmaAndrei MurariuNo ratings yet
- Cardiology STEMIDocument1 pageCardiology STEMIAishwarya WadikarNo ratings yet
- Assignment On Antibiotics - ViosDocument8 pagesAssignment On Antibiotics - ViosIra Velle ViosNo ratings yet
- DRUG STUDY (Groupings) - YASMIEN MARIEDocument21 pagesDRUG STUDY (Groupings) - YASMIEN MARIEYasmien MarieNo ratings yet
- Medical Emergencies Handouts KhannaDocument15 pagesMedical Emergencies Handouts KhannaharryNo ratings yet
- Luka Bakar Poster PDFDocument1 pageLuka Bakar Poster PDFnurisumirizqiNo ratings yet
- Drug Study ICUDocument2 pagesDrug Study ICUErryl Justine AdvinculaNo ratings yet
- Acute Asthma ExacerbationDocument2 pagesAcute Asthma ExacerbationChinenye ModestaNo ratings yet
- Asystole/PEA: Epinephrine 0.1 ML/KG ASAPDocument1 pageAsystole/PEA: Epinephrine 0.1 ML/KG ASAPAlejandro MusaNo ratings yet
- Acs PDFDocument1 pageAcs PDFPowool LalaNo ratings yet
- Ncp-Drug StudyDocument2 pagesNcp-Drug StudyMark oliver GonzalesNo ratings yet
- GROUP1 Drug Therapeutic RecordDocument6 pagesGROUP1 Drug Therapeutic RecordYori Nicole Martine CuyosNo ratings yet
- Asthma and Inhaler 20201203Document29 pagesAsthma and Inhaler 20201203松山內科部No ratings yet
- NCP Rds 2Document1 pageNCP Rds 2Angelokeizer Gavino0% (1)
- Asthma WorksheetDocument5 pagesAsthma WorksheetÀi ZìjǐNo ratings yet
- Adenosine: Facial Flushing, SweatingDocument26 pagesAdenosine: Facial Flushing, SweatingAnna Sofia ReyesNo ratings yet
- Asthma (Acute) Management - Children (Pediatrics)Document2 pagesAsthma (Acute) Management - Children (Pediatrics)Itharshan IndreswaranNo ratings yet
- BCCH ED Croup Algorithm 2012Document1 pageBCCH ED Croup Algorithm 2012john morzNo ratings yet
- COVID - Management 14 April 2021Document20 pagesCOVID - Management 14 April 2021Zain ZaidiNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- Emergency Department Procedural Sedation and Analgesia Physician ChecklistDocument2 pagesEmergency Department Procedural Sedation and Analgesia Physician ChecklistcalstudyNo ratings yet
- Nicolas, Krizha-Drug StudyDocument12 pagesNicolas, Krizha-Drug StudyKrizha Angela NicolasNo ratings yet
- Assessment Nursing Diagnosis Planning Intervention Rationale EvaluationDocument7 pagesAssessment Nursing Diagnosis Planning Intervention Rationale EvaluationEula ReyesNo ratings yet
- Drug Study: Sympathomime Tic, Beta2-Selective Adrenergic Agonist, Bronchodilator, AntiasthmaticDocument3 pagesDrug Study: Sympathomime Tic, Beta2-Selective Adrenergic Agonist, Bronchodilator, AntiasthmaticJichutreasure100% (1)
- Drug StudyDocument22 pagesDrug StudyShenna RegaspiNo ratings yet
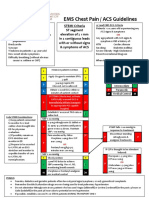
- EMS Chest Pain / ACS GuidelinesDocument1 pageEMS Chest Pain / ACS GuidelinesJuanaly BadiolaNo ratings yet
- Respi Drugs 1Document10 pagesRespi Drugs 1TpdNo ratings yet
- AsthmaDocument2 pagesAsthmaNurliyana GhazaliNo ratings yet
- Procedural SedationDocument9 pagesProcedural SedationZayar SweNo ratings yet
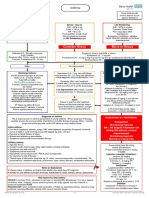
- Managing Acute Asthma in Adults - Final160123Document1 pageManaging Acute Asthma in Adults - Final160123Stri LokaNo ratings yet
- Risk For Ineffective Airway Clearance 1Document8 pagesRisk For Ineffective Airway Clearance 1kint manlangitNo ratings yet
- Croup Summary PDFDocument2 pagesCroup Summary PDFnurfitriaNo ratings yet
- Pediatric Guidelines: Head and Neck Infections - MastoiditisDocument3 pagesPediatric Guidelines: Head and Neck Infections - MastoiditisJr SparkNo ratings yet
- AclsDocument1 pageAclsJoice DasNo ratings yet
- F-IMNCI Chart BookletDocument45 pagesF-IMNCI Chart BookletGunda SrinivasNo ratings yet
- AAH v2 Acute AsthmaDocument81 pagesAAH v2 Acute AsthmaEssa SmjNo ratings yet
- Generalised Ultimate Loads For Pile GroupsDocument22 pagesGeneralised Ultimate Loads For Pile GroupsValerioNo ratings yet
- Course Specifications: Fire Investigation and Failure Analysis (E901313)Document2 pagesCourse Specifications: Fire Investigation and Failure Analysis (E901313)danateoNo ratings yet
- DGA Furan AnalysisDocument42 pagesDGA Furan AnalysisShefian Md Dom100% (10)
- Tours and Travel MNGTDocument16 pagesTours and Travel MNGTArpita Jaiswal100% (5)
- Trandsend 2Document3 pagesTrandsend 2dadiNo ratings yet
- Teacher Resource Disc: Betty Schrampfer Azar Stacy A. HagenDocument10 pagesTeacher Resource Disc: Betty Schrampfer Azar Stacy A. HagenRaveli pieceNo ratings yet
- Read The Text and Answer The QuestionsDocument5 pagesRead The Text and Answer The QuestionsDanny RuedaNo ratings yet
- GP 43-45-DRAFT - Site RestorationDocument48 pagesGP 43-45-DRAFT - Site Restorationmengelito almonte100% (1)
- Transportation Engineering Unit I Part I CTLPDocument60 pagesTransportation Engineering Unit I Part I CTLPMadhu Ane NenuNo ratings yet
- MY-SDK-10000-EE-005 - Method Statement For Concrete Pole Installation - GVB Rev1Document7 pagesMY-SDK-10000-EE-005 - Method Statement For Concrete Pole Installation - GVB Rev1Seeths NairNo ratings yet
- The Way of The Samurai, Shadowrun BookDocument19 pagesThe Way of The Samurai, Shadowrun BookBraedon Montgomery100% (8)
- E10.unit 3 - Getting StartedDocument2 pagesE10.unit 3 - Getting Started27. Nguyễn Phương LinhNo ratings yet
- What Is The Effective Method For Dissolution of HDPE and LDPE - PDFDocument12 pagesWhat Is The Effective Method For Dissolution of HDPE and LDPE - PDFAliNo ratings yet
- Jose André Morales, PH.D.: Ingeniería SocialDocument56 pagesJose André Morales, PH.D.: Ingeniería SocialJYMYNo ratings yet
- Opening The Third EyeDocument13 pagesOpening The Third EyekakamacgregorNo ratings yet
- Python PyDocument19 pagesPython Pyakhilesh kr bhagatNo ratings yet
- Perrys Chemical Engineering Handbook 7th Edition PriceDocument3 pagesPerrys Chemical Engineering Handbook 7th Edition PriceSteven Valentius0% (12)
- Esp-2000 BSDocument6 pagesEsp-2000 BSByron LopezNo ratings yet
- Practice Problems For Modulus and Logarithm Section-I: FiitjeeDocument8 pagesPractice Problems For Modulus and Logarithm Section-I: FiitjeePratham SharmaNo ratings yet
- Hung201 PDFDocument14 pagesHung201 PDFMua Dong Tuyet RoiNo ratings yet
- Updated PDPDocument540 pagesUpdated PDPnikulaaaasNo ratings yet
- My Report in Assessment 1Document67 pagesMy Report in Assessment 1Eddie Wilson BroquezaNo ratings yet
- Put Them Into A Big Bowl. Serve The Salad in Small Bowls. Squeeze Some Lemon Juice. Cut The Fruits Into Small Pieces. Wash The Fruits. Mix The FruitsDocument2 pagesPut Them Into A Big Bowl. Serve The Salad in Small Bowls. Squeeze Some Lemon Juice. Cut The Fruits Into Small Pieces. Wash The Fruits. Mix The FruitsNithya SweetieNo ratings yet
- E34-1 Battery Charging and Dishcharging BoardDocument23 pagesE34-1 Battery Charging and Dishcharging BoardGanesa MurthyNo ratings yet
- English ExerciseDocument2 pagesEnglish ExercisePankhuri Agarwal100% (1)
- Mineral Claim Purchase and Sale Agreement FinalDocument5 pagesMineral Claim Purchase and Sale Agreement Finaldaks4uNo ratings yet
- EverServ 7700 M77XX Quick Reference GuideDocument2 pagesEverServ 7700 M77XX Quick Reference GuidetangocharliepdxNo ratings yet
- Mechanical Power FormulaDocument9 pagesMechanical Power FormulaEzeBorjesNo ratings yet
- Lesson Plan Cot1Document9 pagesLesson Plan Cot1Paglinawan Al KimNo ratings yet
- W1 - V1 MultipleWorksheets SolnDocument3 pagesW1 - V1 MultipleWorksheets SolnAKHIL RAJ SNo ratings yet