You might also like
- Pathology of Alcoholic Liver DiseaseDocument7 pagesPathology of Alcoholic Liver DiseasehghNo ratings yet
- Cholecystitis Concept MapDocument4 pagesCholecystitis Concept Mapnursing concept maps100% (7)
- Revision Notes Dr. A. MowafyDocument222 pagesRevision Notes Dr. A. MowafyMohammed RisqNo ratings yet
- DR - Dilip MMS GIT NotesDocument263 pagesDR - Dilip MMS GIT NotesKoushik Sharma AmancharlaNo ratings yet
- Comparative Animal AnatomyDocument324 pagesComparative Animal AnatomyMohammed Anuz80% (5)
- Chronic Liver Disease (Tutorial)Document44 pagesChronic Liver Disease (Tutorial)Hannah HalimNo ratings yet
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocument42 pagesHepatobiliary Disorders: Katrina Saludar Jimenez, R. NKatrinaJimenezNo ratings yet
- Acute Liver Failure EASL CPGDocument57 pagesAcute Liver Failure EASL CPGFatima Medriza DuranNo ratings yet
- Azolla Success StoryDocument3 pagesAzolla Success StoryThamil ArasanNo ratings yet
- Markiii RM PDFDocument285 pagesMarkiii RM PDFveehneeNo ratings yet
- CKD Case StudyDocument27 pagesCKD Case StudyMary Rose Vito100% (1)
- 06.2 Inborn Error of Metabolism - Iii B - Trans PDFDocument10 pages06.2 Inborn Error of Metabolism - Iii B - Trans PDFAshim AbhiNo ratings yet
- Azolla Study ReportDocument26 pagesAzolla Study ReportThamil ArasanNo ratings yet
- New PPT For HepatitisDocument88 pagesNew PPT For HepatitisPriya100% (1)
- Week 13 NCMB 312 Lect NotesDocument18 pagesWeek 13 NCMB 312 Lect NotesAngie BaylonNo ratings yet
- Imunologie MedicalaDocument224 pagesImunologie MedicalaTo Ma100% (10)
- Duck PDFDocument21 pagesDuck PDFThamil ArasanNo ratings yet
- Hepatobiliary Disorders: Katrina Saludar Jimenez, R. NDocument42 pagesHepatobiliary Disorders: Katrina Saludar Jimenez, R. NreykatNo ratings yet
- Termek Cikk GY0045 1513869631Document7 pagesTermek Cikk GY0045 1513869631ItsAnimal DudeNo ratings yet
- Fulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakyDocument108 pagesFulminant Hepatic Failure (FHF) (Acute Liver Failure (ALF) ) : DR / Reyad AlfakypadmaNo ratings yet
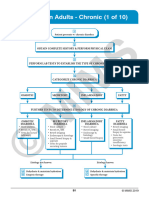
- 62 DiarrheaChronic MGHG MIMG MFM 20161229Document10 pages62 DiarrheaChronic MGHG MIMG MFM 20161229Wei HangNo ratings yet
- Sas S9Document9 pagesSas S9Ralph Louie ManagoNo ratings yet
- 1-Differential Diagnosis of Vomiting 2021 PsáderR SAM3Document28 pages1-Differential Diagnosis of Vomiting 2021 PsáderR SAM3Simay KızılkayaNo ratings yet
- Acute Liver FailureDocument53 pagesAcute Liver FailureMonesh-BhaskaranNo ratings yet
- Prolonged Cholestasis Due To Hepatitis A Virus Infection in A Young Adolescent Male With A Known Case of Hemoglobin E Disease: Early Response To Steroid TherapyDocument4 pagesProlonged Cholestasis Due To Hepatitis A Virus Infection in A Young Adolescent Male With A Known Case of Hemoglobin E Disease: Early Response To Steroid TherapyBOHR International Journal on GastroenterologyNo ratings yet
- Cushings-Pt2 (2021 - 03 - 03 15 - 11 - 26 UTC)Document8 pagesCushings-Pt2 (2021 - 03 - 03 15 - 11 - 26 UTC)magloria77No ratings yet
- Jaundice and Ascites Group ProjectDocument15 pagesJaundice and Ascites Group ProjectJosiah Noella BrizNo ratings yet
- Review: Liver Dysfunction in Critical IllnessDocument17 pagesReview: Liver Dysfunction in Critical IllnessRoger Ludeña SalazarNo ratings yet
- Sa Jun 2018 PDFDocument6 pagesSa Jun 2018 PDFdpcamposhNo ratings yet
- 3939 Whitcomb CRNP AGA Aug2014Document27 pages3939 Whitcomb CRNP AGA Aug2014Leopoldo MagañaNo ratings yet
- Acute Glomerular Nephritis V.S Nephrotic SyndromeDocument4 pagesAcute Glomerular Nephritis V.S Nephrotic SyndromeYoussef AliNo ratings yet
- NCMB312 LECTURE: Communicable Diseases, Cancer, Nursing CareDocument63 pagesNCMB312 LECTURE: Communicable Diseases, Cancer, Nursing CareRose Ann CammagayNo ratings yet
- CLD FinalDocument17 pagesCLD FinalHervis FantiniNo ratings yet
- Gastrointestinal System (Paper-V) PBQs 2018 KU With SolutionsDocument6 pagesGastrointestinal System (Paper-V) PBQs 2018 KU With SolutionsCatalyst NepalNo ratings yet
- LiverDocument30 pagesLiverNisini ImanyaNo ratings yet
- Case Study in Vesicovaginal FistulaDocument14 pagesCase Study in Vesicovaginal FistulaIvory100% (4)
- Model Test-1 SolveDocument20 pagesModel Test-1 SolveRaihanShaheedNo ratings yet
- I Patient Assessment Data BaseDocument12 pagesI Patient Assessment Data BaseJanice_Fernand_1603No ratings yet
- Pharmacology LaqDocument11 pagesPharmacology Laqravindra b kadamNo ratings yet
- Final Neonatal JaundiceDocument47 pagesFinal Neonatal JaundiceArati JhaNo ratings yet
- Management of Severe Malaria in Pregnancy-Final 2Document30 pagesManagement of Severe Malaria in Pregnancy-Final 2ocencolumbusNo ratings yet
- Viral Diseases of Alimentary Canal in CaninesDocument37 pagesViral Diseases of Alimentary Canal in CaninesNavneet BajwaNo ratings yet
- Pediatric Hepatitis - General PrinciplesDocument52 pagesPediatric Hepatitis - General Principlesesra yulianaNo ratings yet
- Case Presentation Febrile Neutropenia NizarDocument25 pagesCase Presentation Febrile Neutropenia NizarNizar IJNo ratings yet
- Elevated Deoxycholic Acid and Idiopathic Recurrent Acute PancreatitisDocument3 pagesElevated Deoxycholic Acid and Idiopathic Recurrent Acute PancreatitisMaria LimaNo ratings yet
- Management of DiarrheaDocument12 pagesManagement of DiarrheaHammo Ez AldienNo ratings yet
- Viral Hepatitis and Alcoholic Liver Disease: Prepared By: Azhi Omer - F190219 Supervised By: Dr. Truska FaraidunDocument29 pagesViral Hepatitis and Alcoholic Liver Disease: Prepared By: Azhi Omer - F190219 Supervised By: Dr. Truska FaraidunMustafa Salam M.NooriNo ratings yet
- 2017-2018 - GI Infectious DiseasesDocument57 pages2017-2018 - GI Infectious Diseasesbahadar94No ratings yet
- 2.4.4.3D Reye's Syndrome - Dr. SaptinoDocument48 pages2.4.4.3D Reye's Syndrome - Dr. Saptinonawal asmadiNo ratings yet
- Analytical Study of Pancreatitis in DogsDocument4 pagesAnalytical Study of Pancreatitis in DogsMaria Isabel GomezNo ratings yet
- Minimizing Bleeding: Late SignDocument12 pagesMinimizing Bleeding: Late SignMatth N. ErejerNo ratings yet
- Alf Ajay AgadeDocument84 pagesAlf Ajay AgadeVinay PatilNo ratings yet
- Hepatitis GeneralDocument14 pagesHepatitis GeneralMarysol UlloaNo ratings yet
- 04 FCH Acute GastroenteritisDocument9 pages04 FCH Acute GastroenteritisClar MoniquezNo ratings yet
- Antibiotics by Clinical CasesDocument59 pagesAntibiotics by Clinical CasesNikNo ratings yet
- PYELONEPHRITISDocument1 pagePYELONEPHRITISgreskpremium8No ratings yet
- JAUNDICE - Role PlayDocument2 pagesJAUNDICE - Role Playnathanaellee92No ratings yet
- Jaundice 160318164012Document47 pagesJaundice 160318164012Ritik MishraNo ratings yet
- Harriet Lane Handbook 21st Ed 2018-401-600Document200 pagesHarriet Lane Handbook 21st Ed 2018-401-600nguyễn vjNo ratings yet
- Vit B (FSW)Document2 pagesVit B (FSW)khelxoNo ratings yet
- Top 5 Breed-Associated Biochemical AbnormalitiesDocument5 pagesTop 5 Breed-Associated Biochemical AbnormalitiesCabinet VeterinarNo ratings yet
- Ptyalism & Pseudoptyalism - Allen, JulieDocument2 pagesPtyalism & Pseudoptyalism - Allen, JulieJuanMartínezNo ratings yet
- RCPCH guidance on rare inflammatory syndrome in childrenDocument6 pagesRCPCH guidance on rare inflammatory syndrome in childrenMario TGNo ratings yet
- Liver Focus 20Document7 pagesLiver Focus 20Sanja CirkovicNo ratings yet
- Case Study Tumor LysisDocument28 pagesCase Study Tumor Lysisapi-653850652No ratings yet
- Feline BabesiosisDocument8 pagesFeline BabesiosisPretty PeterNo ratings yet
- Unit - I: Managee's Potential Is Determined When A Set of Tasks Are Assigned To Him. It IsDocument233 pagesUnit - I: Managee's Potential Is Determined When A Set of Tasks Are Assigned To Him. It IsAmit BaruahNo ratings yet
- How Estrogen Protects BonesDocument7 pagesHow Estrogen Protects BonesThamil ArasanNo ratings yet
- 5 OzkanDocument6 pages5 OzkanThamil ArasanNo ratings yet
- Interglobe Aviation LTDDocument2 pagesInterglobe Aviation LTDThamil ArasanNo ratings yet
- Agriculture Knowledge Management: Advance Training Program OnDocument68 pagesAgriculture Knowledge Management: Advance Training Program OnThamil ArasanNo ratings yet
- Equine ExamDocument85 pagesEquine Examياسر قاتل البزونNo ratings yet
- Anesthesia Guidelines For Dogs and CatsDocument9 pagesAnesthesia Guidelines For Dogs and CatsNatalie KingNo ratings yet
- How 20to 20perform 20a 20physical 20exam 20in 20your 20horseDocument50 pagesHow 20to 20perform 20a 20physical 20exam 20in 20your 20horseThamil ArasanNo ratings yet
- Ivra Abstracts 2012Document42 pagesIvra Abstracts 2012Thamil ArasanNo ratings yet
- Byagagaire - Xylazine Hydrochloride and Ketamine Hydrochloride Combinations For General Anaesthesia in SheepDocument182 pagesByagagaire - Xylazine Hydrochloride and Ketamine Hydrochloride Combinations For General Anaesthesia in SheepThamil ArasanNo ratings yet
- Infection and ImmunityDocument36 pagesInfection and ImmunityThamil ArasanNo ratings yet
- 3rd Yr CFC Handbook - 2 - Final 2010-11Document16 pages3rd Yr CFC Handbook - 2 - Final 2010-11Barbara LiNo ratings yet
- Anatomy of The Equine FootDocument14 pagesAnatomy of The Equine FootEdmilson Daneze100% (1)
- All Accounts Balance Details: S. No. Account Number Account Type Branch Rate of Interest (% P.a.) BalanceDocument1 pageAll Accounts Balance Details: S. No. Account Number Account Type Branch Rate of Interest (% P.a.) BalanceThamil ArasanNo ratings yet
- Bone Marrow Sampling: Bone Marrow Cytology (Aspiration) Vs Histology (Core Biopsy)Document5 pagesBone Marrow Sampling: Bone Marrow Cytology (Aspiration) Vs Histology (Core Biopsy)Thamil ArasanNo ratings yet
- Hanuman Chalisa Lyrics in Tamil Font PDFDocument4 pagesHanuman Chalisa Lyrics in Tamil Font PDFThamil ArasanNo ratings yet
- Caesarean SectionDocument1 pageCaesarean SectionThamil ArasanNo ratings yet
- Duck Housing and ManagementDocument7 pagesDuck Housing and ManagementThamil ArasanNo ratings yet
- Adoption of Azolla Cultivation Technology in The Farmers' Field: An AnalysisDocument7 pagesAdoption of Azolla Cultivation Technology in The Farmers' Field: An AnalysisThamil ArasanNo ratings yet
- AO - Dental Prophylaxis in A DogDocument5 pagesAO - Dental Prophylaxis in A DogThamil ArasanNo ratings yet
- MYD - Hematochezia in A DogDocument5 pagesMYD - Hematochezia in A DogThamil ArasanNo ratings yet
- Imcrj 9 241Document5 pagesImcrj 9 241Thamil ArasanNo ratings yet
- Azolla Cultivation and Feeding LivestockDocument1 pageAzolla Cultivation and Feeding LivestockThamil ArasanNo ratings yet
- 1 s2.0 S0168827820304700 MainDocument11 pages1 s2.0 S0168827820304700 MainHadi KuriryNo ratings yet
- Complicaciones y Costos de La Biopsia HepaticaDocument9 pagesComplicaciones y Costos de La Biopsia HepaticaYonatan Merchant PerezNo ratings yet
- Non Invasive Imaging in NASHDocument3 pagesNon Invasive Imaging in NASHParul SoodNo ratings yet
- Fibroscan Interpretation - Guide 2020Document2 pagesFibroscan Interpretation - Guide 2020Faisal BaigNo ratings yet
- Hepatitis BDocument61 pagesHepatitis BMichael AmandyNo ratings yet
- PAPAS Predict Liver FibrosisDocument7 pagesPAPAS Predict Liver Fibrosisemilya007No ratings yet
- Sammons 2014Document5 pagesSammons 2014viviana castillo VanegasNo ratings yet
- Cirrosis BMJDocument91 pagesCirrosis BMJJuan Luis Nuñez AravenaNo ratings yet
- Noninvasive Assessment of Hepatic Fibrosis - Overview of Serologic Tests and Imaging Examinations - UpToDateDocument35 pagesNoninvasive Assessment of Hepatic Fibrosis - Overview of Serologic Tests and Imaging Examinations - UpToDatepopasorinemilianNo ratings yet
- Portal HypertensionDocument13 pagesPortal HypertensionCiprian BoesanNo ratings yet
- Liver Curs 2009Document215 pagesLiver Curs 2009Mohammad_Islam87No ratings yet
- The Perils of Fatty Liver Disease: Linical Aboratory EwsDocument20 pagesThe Perils of Fatty Liver Disease: Linical Aboratory EwsamirohkurniatiNo ratings yet
- Editorial Commentary On The Indian Journal of Gastroenterology May-June 2020Document3 pagesEditorial Commentary On The Indian Journal of Gastroenterology May-June 2020sivagiri.pNo ratings yet
- The Almost-Normal Liver Biopsy: Presentation, Clinical Associations, and OutcomeDocument7 pagesThe Almost-Normal Liver Biopsy: Presentation, Clinical Associations, and OutcomeAntonio RolonNo ratings yet
- Download ebook Scheuers Liver Biopsy Interpretation Pdf full chapter pdfDocument67 pagesDownload ebook Scheuers Liver Biopsy Interpretation Pdf full chapter pdfwilliam.balasco829100% (23)
- Liver BiopsyDocument4 pagesLiver BiopsyLouis FortunatoNo ratings yet
- Cirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDate PDFDocument33 pagesCirrhosis in Adults - Etiologies, Clinical Manifestations, and Diagnosis - UpToDate PDFDonto KonoNo ratings yet
- Guidelines On Prevention of Bleeding and Thrombosis in Cirrhosis-1Document34 pagesGuidelines On Prevention of Bleeding and Thrombosis in Cirrhosis-1labertoNo ratings yet
- Hepatomegali in Infant and Children - Pediatrics in Review-2000-Wolf-303-10Document10 pagesHepatomegali in Infant and Children - Pediatrics in Review-2000-Wolf-303-10Reddy LufyanNo ratings yet
- Hepatic, Pancreatic, and Rare Gastrointestinal Complications of Immune Checkpoint Inhibitor Therapy - UpToDateDocument29 pagesHepatic, Pancreatic, and Rare Gastrointestinal Complications of Immune Checkpoint Inhibitor Therapy - UpToDatemayteveronica1000No ratings yet
- Liver Biopsy: Mary Raina Angeli Fujiyoshi, MDDocument10 pagesLiver Biopsy: Mary Raina Angeli Fujiyoshi, MDRaina FujiyoshiNo ratings yet
- PIIS019096222030284XDocument42 pagesPIIS019096222030284XSafira Rosyadatul AissyNo ratings yet
- Case 4 - 2023Document11 pagesCase 4 - 2023Katherine VadilloNo ratings yet
- Europass Curriculum Vitae: Personal Information Popescu Simona-AlinaDocument11 pagesEuropass Curriculum Vitae: Personal Information Popescu Simona-AlinaTanveerNo ratings yet
- Metabolism and EndocrineDocument156 pagesMetabolism and EndocrineGren May Angeli MagsakayNo ratings yet
- Liver Fibrosis A Compilation On The Biomarkers StaDocument17 pagesLiver Fibrosis A Compilation On The Biomarkers Stamy accountNo ratings yet
- FibroscanDocument3 pagesFibroscanAri WirantariNo ratings yet
- Nurc Gastrointestinal Hepatobiliary & Neurological Nursing: Masmunaa Hassan 19 September 2017Document29 pagesNurc Gastrointestinal Hepatobiliary & Neurological Nursing: Masmunaa Hassan 19 September 2017Jakub KubaNo ratings yet
- Ferritin As An Indices of Body Iron Stores and Acute Myocardeal Infarction in DiabeticsDocument58 pagesFerritin As An Indices of Body Iron Stores and Acute Myocardeal Infarction in DiabeticsJagannadha Rao PeelaNo ratings yet