You might also like
- The DIRKS Methodology: A User GuideDocument285 pagesThe DIRKS Methodology: A User GuideJesus Frontera100% (2)
- Chapter 33 Guyton and HallDocument4 pagesChapter 33 Guyton and Hallg_komolafeNo ratings yet
- Patton and Thibodeau: Anthony's Textbook of Anatomy & Physiology, 19 EditionDocument1 pagePatton and Thibodeau: Anthony's Textbook of Anatomy & Physiology, 19 Editionllaurennn23No ratings yet
- Physiology Comprehensive Exam Pointers PDFDocument108 pagesPhysiology Comprehensive Exam Pointers PDFRaynalynGimoros100% (1)
- 03f - 8-06 Awake ImagesDocument2 pages03f - 8-06 Awake ImagesRobert CamachoNo ratings yet
- Biology Assignment (Stem Cells)Document3 pagesBiology Assignment (Stem Cells)Dwayne CoelhoNo ratings yet
- Ford Focus MK2 Headlight Switch Wiring DiagramDocument1 pageFord Focus MK2 Headlight Switch Wiring DiagramAdam TNo ratings yet
- API RP 7C-11F Installation, Maintenance and Operation of Internal Combustion Engines.Document3 pagesAPI RP 7C-11F Installation, Maintenance and Operation of Internal Combustion Engines.Rashid Ghani100% (1)
- Hemopoiesis PDFDocument14 pagesHemopoiesis PDFrysnawahyu13No ratings yet
- Lecture 1 - Introduction To HematologyDocument30 pagesLecture 1 - Introduction To Hematologyimam100% (1)
- HIS.K.1.Histology of BloodDocument16 pagesHIS.K.1.Histology of BloodMayaPasaribuNo ratings yet
- 2.1 RESISTANCE OF THE BODY TO INFECTION I Leukocytes GranulocytesDocument40 pages2.1 RESISTANCE OF THE BODY TO INFECTION I Leukocytes GranulocytesGeevee Naganag VentulaNo ratings yet
- Oo GenesisDocument20 pagesOo GenesisDinar Yudistira FirdausNo ratings yet
- Blood Cells, Immunity and Blood ClottingDocument65 pagesBlood Cells, Immunity and Blood Clottingmunaamuummee100% (1)
- MetaplasiaDocument6 pagesMetaplasiaMd Ahsanuzzaman PinkuNo ratings yet
- Metamorphosis in InsectsDocument13 pagesMetamorphosis in InsectsAnupam GhoshNo ratings yet
- APP2 E1 NoteDocument28 pagesAPP2 E1 NotelifecostNo ratings yet
- Physiology L6Document6 pagesPhysiology L6Anonymous elq7jZiSNo ratings yet
- Blood ComponentsDocument17 pagesBlood ComponentsJohnSmithNo ratings yet
- Lymphoid Organs (Primary Lympoid Organ)Document10 pagesLymphoid Organs (Primary Lympoid Organ)KarthigaNo ratings yet
- Frog Embryo PDFDocument17 pagesFrog Embryo PDFmicrobeateria100% (1)
- Enzymology: Discuss About Regulation of Enzyme ActivityDocument4 pagesEnzymology: Discuss About Regulation of Enzyme ActivityNorrifhan Akmal IsmailNo ratings yet
- Intrdoduction Gis 2 (Associated Organs) : Maya Tejasari Histology DepartmentDocument24 pagesIntrdoduction Gis 2 (Associated Organs) : Maya Tejasari Histology DepartmentIpan YustiartaNo ratings yet
- The Complement SystemDocument24 pagesThe Complement Systemhkatniwala100% (1)
- BloodDocument38 pagesBloodchukwukerechimezirimNo ratings yet
- Mitosis and MeiosisDocument13 pagesMitosis and Meiosis420192420192No ratings yet
- Cell Division Mitosis MeiosisDocument49 pagesCell Division Mitosis MeiosisKeaneNo ratings yet
- THROMBOSISDocument18 pagesTHROMBOSISShruti Verma100% (1)
- Endocytosis ExocytosisDocument5 pagesEndocytosis ExocytosisMiska Fairuz100% (1)
- Endo 3 Notes PDFDocument9 pagesEndo 3 Notes PDFDilNo ratings yet
- Body Fluids and Fluid Compartments: Subject AboutDocument10 pagesBody Fluids and Fluid Compartments: Subject AboutHareth mohammad mahmod NawajaNo ratings yet
- 200L Excitable Tissues & Ans PhysiologyDocument65 pages200L Excitable Tissues & Ans PhysiologyAdedolapo bello100% (1)
- Overview of Cell Cycle by Javali.GDocument15 pagesOverview of Cell Cycle by Javali.GJavali.GNo ratings yet
- Thyroid Pathophysiology and Diagnostic Evaluation: Chapter OutlineDocument38 pagesThyroid Pathophysiology and Diagnostic Evaluation: Chapter OutlinePedro Gómez RNo ratings yet
- Kuliah BMD Pathomechanism DemaDocument30 pagesKuliah BMD Pathomechanism DemaSelebriti Indonesia100% (1)
- Apoptosis PDFDocument67 pagesApoptosis PDFmkman100% (1)
- 3rd Lecture On Skeletal Muscle Physiology by DR - RoomiDocument21 pages3rd Lecture On Skeletal Muscle Physiology by DR - RoomiMudassar Roomi67% (3)
- APHERESISDocument9 pagesAPHERESISSiti Zulaikha ZulaikhaNo ratings yet
- Polytene and Lampbrush ChromosomesDocument3 pagesPolytene and Lampbrush Chromosomesneeru.bhagatNo ratings yet
- Lymphatic Organs and TissuesDocument3 pagesLymphatic Organs and TissuesSaman Bharatha KotigalaNo ratings yet
- Complement System: Pathways, Functions and RegulationDocument6 pagesComplement System: Pathways, Functions and RegulationN.vijaykanthNo ratings yet
- C19 2 Hemopoiesis Eythropoiesis LeukopoiesisDocument11 pagesC19 2 Hemopoiesis Eythropoiesis Leukopoiesisnurul azisyah auraNo ratings yet
- Cell Structure IDocument64 pagesCell Structure IDwi Puji Astini100% (1)
- Function of RBCDocument9 pagesFunction of RBCAthea MelosantosNo ratings yet
- Malaria ParasiteDocument22 pagesMalaria ParasiteAndy Putra HermawanNo ratings yet
- Reproductive System Male and FemaleDocument61 pagesReproductive System Male and FemaleAsad KHAN100% (1)
- White Blood Cells (WBC) PDFDocument3 pagesWhite Blood Cells (WBC) PDFPerry SinNo ratings yet
- 04 First Week of DevelopmentDocument70 pages04 First Week of DevelopmentOsman Saidu SesayNo ratings yet
- Ligand and Cell Signaling PathwaysDocument117 pagesLigand and Cell Signaling PathwaysShoaib MomenNo ratings yet
- Psilophyta To SphenophytaDocument39 pagesPsilophyta To Sphenophytajaninamariesarmiento100% (1)
- Oogenesis and Ovarian Cycle, Uterus, Menstrual Cycle ABORTION TERATOLOGYDocument72 pagesOogenesis and Ovarian Cycle, Uterus, Menstrual Cycle ABORTION TERATOLOGYElizabeth OmobolanleNo ratings yet
- Bone Tissues 1Document38 pagesBone Tissues 1ms_pianist100% (1)
- Leukocytes, Granulocytes, The Monocyte-Macrophage System, and InflammationDocument10 pagesLeukocytes, Granulocytes, The Monocyte-Macrophage System, and InflammationShi no MeNo ratings yet
- Dr. Khairun Nisa, Mkes., AIFO Fakultas Kedokteran Universitas Lampung 2014Document35 pagesDr. Khairun Nisa, Mkes., AIFO Fakultas Kedokteran Universitas Lampung 2014Riska WulandariNo ratings yet
- The Eukaryotic Genome andDocument76 pagesThe Eukaryotic Genome andKehkashan KhanNo ratings yet
- Path Phys4Document73 pagesPath Phys4Наталія Вікторівна ДавиденкоNo ratings yet
- Notes - Growth and DevelopmentDocument4 pagesNotes - Growth and DevelopmentNathan mwapeNo ratings yet
- Blood 12-6-2018Document42 pagesBlood 12-6-2018Noor Fatima100% (1)
- Cell Cycle Cell Division PDFDocument13 pagesCell Cycle Cell Division PDFmuzamil shabir100% (1)
- Taste SensationDocument56 pagesTaste SensationSyedaNaveenBatoolNo ratings yet
- Bone Marrow and Hematopoiesis - 2Document7 pagesBone Marrow and Hematopoiesis - 2Sharan MurugaboopathyNo ratings yet
- Bio 2 Assignment 3Document16 pagesBio 2 Assignment 3Arun RajNo ratings yet
- BSC Lecture Notes Semester 1Document7 pagesBSC Lecture Notes Semester 1satasha28No ratings yet
- Gliadel Wafer sNDA 20-637s: Guilford Pharmaceuticals Inc. Baltimore, MarylandDocument91 pagesGliadel Wafer sNDA 20-637s: Guilford Pharmaceuticals Inc. Baltimore, MarylandVikram KumarNo ratings yet
- Allergic RhinitisDocument3 pagesAllergic RhinitisVikram KumarNo ratings yet
- Ascot TrialDocument26 pagesAscot TrialVikram Kumar0% (1)
- Adl - 16 TQMDocument7 pagesAdl - 16 TQMVikram KumarNo ratings yet
- Marketing Mix PDFDocument20 pagesMarketing Mix PDFVikram KumarNo ratings yet
- Affordability Is The Key To Increase AscessDocument2 pagesAffordability Is The Key To Increase AscessVikram KumarNo ratings yet
- Aroicon 2011Document1 pageAroicon 2011Vikram KumarNo ratings yet
- Demand Forecasting: Evidence-Based Methods: Armstrong@wharton - Upenn.eduDocument23 pagesDemand Forecasting: Evidence-Based Methods: Armstrong@wharton - Upenn.eduChuka ChumaNo ratings yet
- Breast Cancer AwarenessDocument14 pagesBreast Cancer AwarenessVikram KumarNo ratings yet
- Mba Eft 1st Sems.Document5 pagesMba Eft 1st Sems.Vikram KumarNo ratings yet
- Delhi Schools Nursery Admissions Schedule 2012 27 Dec 7AM1Document108 pagesDelhi Schools Nursery Admissions Schedule 2012 27 Dec 7AM1Vikram KumarNo ratings yet
- Marketing Budget Allocation Techniques HBR ArticleDocument46 pagesMarketing Budget Allocation Techniques HBR ArticleVinoth_iimrNo ratings yet
- 4164315024Document1 page4164315024Vikram KumarNo ratings yet
- Polyether Polyol Production AssignmentDocument9 pagesPolyether Polyol Production AssignmentanurdiaNo ratings yet
- Entrepreneurship - PPTX Version 1 - Copy (Autosaved) (Autosaved) (Autosaved) (Autosaved)Document211 pagesEntrepreneurship - PPTX Version 1 - Copy (Autosaved) (Autosaved) (Autosaved) (Autosaved)Leona Alicpala67% (3)
- CV Ashish PDFDocument3 pagesCV Ashish PDFRoshan KejariwalNo ratings yet
- Capgemini - 2012-06-13 - 2012 Analyst Day - 3 - Michelin - A Better Way ForwardDocument12 pagesCapgemini - 2012-06-13 - 2012 Analyst Day - 3 - Michelin - A Better Way ForwardAvanish VermaNo ratings yet
- Electronics 11 02566Document13 pagesElectronics 11 02566卓七越No ratings yet
- How To Change Front Suspension Strut On Citroen Xsara Coupe n0 Replacement GuideDocument25 pagesHow To Change Front Suspension Strut On Citroen Xsara Coupe n0 Replacement Guidematej89No ratings yet
- Outlook of PonDocument12 pagesOutlook of Ponty nguyenNo ratings yet
- Corelink Mmu600ae TRM 101412 0100 00 enDocument194 pagesCorelink Mmu600ae TRM 101412 0100 00 enLv DanielNo ratings yet
- Vest3000mkii TurntableDocument16 pagesVest3000mkii TurntableElkin BabiloniaNo ratings yet
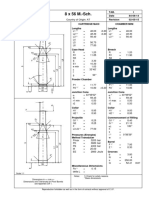
- 8 X 56 M.-SCH.: Country of Origin: ATDocument1 page8 X 56 M.-SCH.: Country of Origin: ATMohammed SirelkhatimNo ratings yet
- Fuentes v. Office of The Ombudsman - MindanaoDocument6 pagesFuentes v. Office of The Ombudsman - MindanaoJ. JimenezNo ratings yet
- EC 2012 With SolutionsDocument50 pagesEC 2012 With Solutionsprabhjot singh1No ratings yet
- City Limits Magazine, December 1981 IssueDocument28 pagesCity Limits Magazine, December 1981 IssueCity Limits (New York)No ratings yet
- Worked Solution Paper5 A LevelDocument8 pagesWorked Solution Paper5 A LevelBhoosan AncharazNo ratings yet
- Handbook of Storage Tank Systems: Codes, Regulations, and DesignsDocument4 pagesHandbook of Storage Tank Systems: Codes, Regulations, and DesignsAndi RachmanNo ratings yet
- 9701 Nos Ps 23Document5 pages9701 Nos Ps 23Hubbak KhanNo ratings yet
- TransistorsDocument21 pagesTransistorsAhmad AzriNo ratings yet
- Blackbook 2Document94 pagesBlackbook 2yogesh kumbharNo ratings yet
- BarricadeDocument6 pagesBarricadeJithu PappachanNo ratings yet
- Kortz Center GTA Wiki FandomDocument1 pageKortz Center GTA Wiki FandomsamNo ratings yet
- 2010 Information ExchangeDocument15 pages2010 Information ExchangeAnastasia RotareanuNo ratings yet
- Communicating Value - PatamilkaDocument12 pagesCommunicating Value - PatamilkaNeha ArumallaNo ratings yet
- WSD M1a283 B50Document9 pagesWSD M1a283 B50'Lampa'No ratings yet
- Norman, K. R., Pali Philology & The Study of BuddhismDocument13 pagesNorman, K. R., Pali Philology & The Study of BuddhismkhrinizNo ratings yet
- ES Parent Bulletin Vol#19 2012 May 25Document13 pagesES Parent Bulletin Vol#19 2012 May 25International School ManilaNo ratings yet
- Department of Education: Raiseplus Weekly Plan For Blended LearningDocument3 pagesDepartment of Education: Raiseplus Weekly Plan For Blended LearningMARILYN CONSIGNANo ratings yet
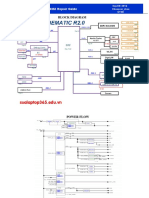
- Asus x453Document5 pagesAsus x453Rhiry Ntuh AthryNo ratings yet