You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Evolution of Lasers: A Delight in Dentistry: Articles GeneralDocument7 pagesEvolution of Lasers: A Delight in Dentistry: Articles Generalshamshuddin patelNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Recognition and Management of Palatogingival GroovDocument10 pagesRecognition and Management of Palatogingival Groovshamshuddin patelNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hero Shaper Final 9Document2 pagesHero Shaper Final 9shamshuddin patelNo ratings yet
- Effect of ProTaper Universal, Endoflare, Revo-S, HyFlexDocument3 pagesEffect of ProTaper Universal, Endoflare, Revo-S, HyFlexshamshuddin patelNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- A Miracle of Flexibility and Fracture Resistance!: The New Niti File GenerationDocument6 pagesA Miracle of Flexibility and Fracture Resistance!: The New Niti File Generationshamshuddin patelNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Canal Configuration in The Mesiobuccal Root of The Maxillary First Molar and Its Endodontic SignificanceDocument7 pagesCanal Configuration in The Mesiobuccal Root of The Maxillary First Molar and Its Endodontic Significanceshamshuddin patelNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A New System For Classifying Root and Root Canal Morphology: ReviewDocument11 pagesA New System For Classifying Root and Root Canal Morphology: Reviewshamshuddin patelNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- O Ehlers 1957Document15 pagesO Ehlers 1957shamshuddin patelNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Ver Tucci 1974Document9 pagesVer Tucci 1974shamshuddin patelNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Accessory Canal PDFDocument13 pagesAccessory Canal PDFshamshuddin patelNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Pagets DiseaseDocument62 pagesPagets DiseaseKush PathakNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Odtp Boards Exam OverviewDocument5 pagesOdtp Boards Exam OverviewAndrew McDonald100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- CPSM Manitoba Methadone & Buprenorphine Maintenance - Recommended PracticeDocument85 pagesCPSM Manitoba Methadone & Buprenorphine Maintenance - Recommended PracticeGNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Sample Size PilotDocument5 pagesSample Size PilotmsriramcaNo ratings yet
- 13.loading of Dental ImplantsDocument166 pages13.loading of Dental ImplantsHarpreet Singh100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Ed GeinDocument4 pagesEd GeinDaniel OxendineNo ratings yet
- Updates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionDocument12 pagesUpdates in The Treatment of Eating Disorders in 2022 A Year in Review in Eating Disorders The Journal of Treatment PreventionMarietta_MonariNo ratings yet
- A Review of Conjoint Family Therapy and The Theories of Virginia SatirDocument9 pagesA Review of Conjoint Family Therapy and The Theories of Virginia SatirLORETO CNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Final Research Thesis Og Milignant HyperthermiaDocument38 pagesFinal Research Thesis Og Milignant HyperthermiaImran MukhlessNo ratings yet
- The Magic of Ilizarov PDFDocument310 pagesThe Magic of Ilizarov PDFOrto Mesp83% (6)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- What Is Maslows Hierarchy of Needs 4136760Document6 pagesWhat Is Maslows Hierarchy of Needs 4136760Pramod ShriwastavaNo ratings yet
- RNI For Malaysians-SummaryDocument2 pagesRNI For Malaysians-SummaryAimi Hannani100% (1)
- Cmagbanua Aicbm Handout 2s 127pDocument127 pagesCmagbanua Aicbm Handout 2s 127pWilliam Tell100% (2)
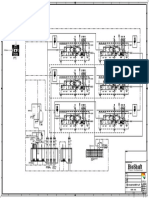
- P&ID - STP-Yanbu SWCC (6units)Document1 pageP&ID - STP-Yanbu SWCC (6units)Ashraf BayomiNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- FAQ About IVT TrainingDocument12 pagesFAQ About IVT TrainingJohanna ChavezNo ratings yet
- Partial MastectomyDocument17 pagesPartial MastectomyJill Rae Lloren ConsolacionNo ratings yet
- Information To Be Included Within A Coal Mining Risk AssessmentDocument2 pagesInformation To Be Included Within A Coal Mining Risk AssessmentAlf HorsemanNo ratings yet
- 3.02 Learning and Memory: ExamplesDocument2 pages3.02 Learning and Memory: ExamplesMarkayla HinesNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- EpulisDocument7 pagesEpulisSean Anderson100% (1)
- FS13 PolycythemiaVera FactSheetDocument7 pagesFS13 PolycythemiaVera FactSheetMala 'emyu' UmarNo ratings yet
- Secondary Angle Closure GlaucomaDocument35 pagesSecondary Angle Closure GlaucomaAndriati NadhilaNo ratings yet
- Embodied PracticeDocument3 pagesEmbodied PracticeOdoroagă AlexandraNo ratings yet
- 7x Premature EjaculationDocument8 pages7x Premature EjaculationTer AbNo ratings yet
- DPA Fact Sheet Portugal Decriminalization Feb2014Document3 pagesDPA Fact Sheet Portugal Decriminalization Feb2014webmaster@drugpolicy.orgNo ratings yet
- Can Coloring Mandalas Reduce AnxietyDocument6 pagesCan Coloring Mandalas Reduce AnxietyAbirNo ratings yet
- Benefits of Zinc:: 1 - Zinc and Regulating Immune FunctionDocument3 pagesBenefits of Zinc:: 1 - Zinc and Regulating Immune FunctionHuda BaharoonNo ratings yet
- The Healthy Bones Nutrition Plan and Cookbook - IntroductionDocument10 pagesThe Healthy Bones Nutrition Plan and Cookbook - IntroductionChelsea Green PublishingNo ratings yet
- OralMeds - ChecklistDocument6 pagesOralMeds - ChecklistXandra BasnilloNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Home Care Catalogue UK Edition 4 Web PDFDocument60 pagesHome Care Catalogue UK Edition 4 Web PDFmanuales tecnicosNo ratings yet
- Preoperative Planning For Primary Total Hip ArthroplastyDocument8 pagesPreoperative Planning For Primary Total Hip Arthroplastyanon_683301094No ratings yet