You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- S/N Cat: Safa Defect Categorization AerospaceDocument36 pagesS/N Cat: Safa Defect Categorization AerospaceZain MaqsoodNo ratings yet
- Royal Jordanian - ReservationDocument6 pagesRoyal Jordanian - ReservationAhmed ElghannamNo ratings yet
- Experimental Investigation On Bituminous Mix Using Coconut CoirDocument8 pagesExperimental Investigation On Bituminous Mix Using Coconut CoirTJPRC PublicationsNo ratings yet
- Modifikacii HP 3Document5 pagesModifikacii HP 3pankituna5487No ratings yet
- Development of Api Grade Linepipe Steels at Saudi Iron & Steel Company, HadeedDocument9 pagesDevelopment of Api Grade Linepipe Steels at Saudi Iron & Steel Company, HadeedPatricio AcuñaNo ratings yet
- Swot Analysis of Tata MotorsDocument2 pagesSwot Analysis of Tata MotorsSouvik MajumderNo ratings yet
- Bitumen Bound Materials GuideDocument131 pagesBitumen Bound Materials Guidelyes100% (1)
- Air Conditioning B767 FedexDocument65 pagesAir Conditioning B767 FedexWalter Jair Rodriguez Munoz (LATAM)100% (1)
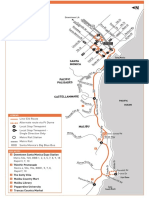
- Route 534 Santa Monica MalibuDocument3 pagesRoute 534 Santa Monica MalibudazulzulNo ratings yet
- XR-71 Oldie SCHDocument1 pageXR-71 Oldie SCHpetskNo ratings yet
- January 21, 2015Document12 pagesJanuary 21, 2015Maple Lake MessengerNo ratings yet
- Bearmach Series3 AccessoriesDocument16 pagesBearmach Series3 AccessoriesscheisshandyNo ratings yet
- Just Plane SmartDocument10 pagesJust Plane Smartnazuwa100% (3)
- Workshop 6 Low Visibility Airport Operations The Tenerife Air Disaster - Individual V1.0Document3 pagesWorkshop 6 Low Visibility Airport Operations The Tenerife Air Disaster - Individual V1.0thao lêNo ratings yet
- Catalogo Resina IngleseDocument9 pagesCatalogo Resina IngleseLevi Franco CarvalhoNo ratings yet
- Managing Products and Services OperationsDocument11 pagesManaging Products and Services OperationsAnne PecadizoNo ratings yet
- RoyalplatinumDocument3 pagesRoyalplatinumRaghavendra KNo ratings yet
- Comprehensive Development Plan 2011 20 FullDocument61 pagesComprehensive Development Plan 2011 20 FullJem SacdalanNo ratings yet
- Crane Safety and Awareness PresentationDocument99 pagesCrane Safety and Awareness Presentationnex1984No ratings yet
- Bibby TopazDocument4 pagesBibby TopazPraveen BalasubramanianNo ratings yet
- Ticket 11 DecDocument2 pagesTicket 11 DecShashank SinghNo ratings yet
- European Green Deal Communication Annex Roadmap - en 1Document4 pagesEuropean Green Deal Communication Annex Roadmap - en 1Nebojsa RedzicNo ratings yet
- Aws WJ 201409Document166 pagesAws WJ 201409spineyro1500No ratings yet
- Warehousing PPT TemplateDocument3 pagesWarehousing PPT TemplateSandip BesraNo ratings yet
- Techn Info Citaro K en LowDocument12 pagesTechn Info Citaro K en Lowwheatly_No ratings yet
- Fact Book March 2021Document64 pagesFact Book March 2021saiNo ratings yet
- Road Qty - S-R-SH-10-Total Project ECL - PCL OffsetDocument1 pageRoad Qty - S-R-SH-10-Total Project ECL - PCL OffsetStephen Rajkumar JayakumarNo ratings yet
- 5Document65 pages5indrajeetNo ratings yet
- Smart Steps Book 3 WebDocument86 pagesSmart Steps Book 3 WebNgaire TaylorNo ratings yet
- SCM Chapter 6Document17 pagesSCM Chapter 6Dito Eri BasyasyaNo ratings yet