You might also like
- (Advances in Cancer Research 114) Ira O. Daar (Eds.) - Guidance Molecules in Cancer and Tumor Angiogenesis-Academic Press, Elsevier (2012)Document273 pages(Advances in Cancer Research 114) Ira O. Daar (Eds.) - Guidance Molecules in Cancer and Tumor Angiogenesis-Academic Press, Elsevier (2012)Mihai MNo ratings yet
- Chughtai 2017Document13 pagesChughtai 2017Mihai MNo ratings yet
- Ligh 2017Document10 pagesLigh 2017Mihai MNo ratings yet
- Emerging Roles of Micrornas in Osteonecrosis of The Femoral HeadDocument6 pagesEmerging Roles of Micrornas in Osteonecrosis of The Femoral HeadMihai MNo ratings yet
- Stages of AnesthesiaDocument3 pagesStages of AnesthesiaMihai MNo ratings yet
- Guo 2017Document6 pagesGuo 2017Mihai MNo ratings yet
- The Current Perspectives of Stem Cell Therapy in Orthopedic SurgeryDocument8 pagesThe Current Perspectives of Stem Cell Therapy in Orthopedic SurgeryMihai MNo ratings yet
- Measure Intracardiac Pressures & Assess Cardiac FunctionDocument41 pagesMeasure Intracardiac Pressures & Assess Cardiac Functionwaleed315No ratings yet
- AutoantibodiesDocument235 pagesAutoantibodiesMihai M100% (2)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Research Paper Outline on Escalation of Opiate UseDocument7 pagesResearch Paper Outline on Escalation of Opiate Usekimwei clintonNo ratings yet
- Republic Act No 9165Document19 pagesRepublic Act No 9165docmabelNo ratings yet
- OpioidsDocument3 pagesOpioidsmuhammadridhwanNo ratings yet
- Oxycodon E: Click To Edit Master Subtitle StyleDocument14 pagesOxycodon E: Click To Edit Master Subtitle StyleKC LawNo ratings yet
- Suboxone - Notes For PharmacistsDocument1 pageSuboxone - Notes For Pharmacistsgarima_montuNo ratings yet
- Toxicology Report For Rapper Lil PeepDocument5 pagesToxicology Report For Rapper Lil PeepKOLD News 13100% (6)
- Opioids MorphineDocument9 pagesOpioids MorphineTueNo ratings yet
- Nervous System and Neurology Assignment - AcrobatiqDocument1 pageNervous System and Neurology Assignment - Acrobatiqjose. medina9No ratings yet
- Fentanyl Fact SheetDocument2 pagesFentanyl Fact SheetSinclair Broadcast Group - EugeneNo ratings yet
- Endo Pharmaceuticals Visual GuideDocument6 pagesEndo Pharmaceuticals Visual GuideDUNCAN0420No ratings yet
- DRUG STUDY - Nalbuphine HydrochlorideDocument2 pagesDRUG STUDY - Nalbuphine HydrochlorideCarson BirthNo ratings yet
- Atestat 1Document22 pagesAtestat 1RalucaxdNo ratings yet
- Penyalahgunaan SuboxoneDocument13 pagesPenyalahgunaan SuboxoneNabellaNo ratings yet
- Stok Benang Kamar OperasiDocument5 pagesStok Benang Kamar OperasirendyNo ratings yet
- Opium - Wikipedia: Images Videos News AnytimeDocument5 pagesOpium - Wikipedia: Images Videos News AnytimedrenevisNo ratings yet
- Antagonists Erses The Effects of Opioid Analgesics by Binding To The Opioid Receptors in The CNS, and IntravenousDocument3 pagesAntagonists Erses The Effects of Opioid Analgesics by Binding To The Opioid Receptors in The CNS, and IntravenousKwin SaludaresNo ratings yet
- Jan-May 2023 SF Medical Examiner Overdose ReportDocument8 pagesJan-May 2023 SF Medical Examiner Overdose ReportCBS News Bay AreaNo ratings yet
- Tag Notes PDFDocument3 pagesTag Notes PDFAlef AminNo ratings yet
- Opioid Conversion Ratios - Guide To Practice 2010: Released December 2010Document12 pagesOpioid Conversion Ratios - Guide To Practice 2010: Released December 2010Ronald WaiNo ratings yet
- Emerging Characteristics of Isotonitazene Involved.14Document3 pagesEmerging Characteristics of Isotonitazene Involved.14ABC Action News50% (2)
- Sketchy OpioidsDocument1 pageSketchy OpioidsSandy MaeNo ratings yet
- Opioid ConversionsDocument3 pagesOpioid Conversionsศักดิ์ชัย พูนศรีเจริญกุลNo ratings yet
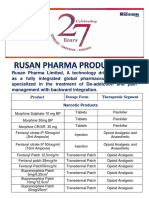
- Rusan Pharma's Pain and Addiction Treatment ProductsDocument4 pagesRusan Pharma's Pain and Addiction Treatment ProductsSanjay SharmaNo ratings yet
- Analgesic Flow ChartDocument2 pagesAnalgesic Flow ChartAtet KurniadiNo ratings yet
- Rekapitulasi Januari 2022Document13 pagesRekapitulasi Januari 2022galiharumNo ratings yet
- Satyanand Sahu (Narcotic and Non - Narcotic Analgesic)Document44 pagesSatyanand Sahu (Narcotic and Non - Narcotic Analgesic)Satyanand SahuNo ratings yet
- Kratom Alkaloid BreakdownDocument3 pagesKratom Alkaloid BreakdownAsif Majeed100% (4)
- Pharmacology of Opioid AnalgesicsDocument64 pagesPharmacology of Opioid AnalgesicsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- NaloxBox Press Event Agenda and News ReleaseDocument5 pagesNaloxBox Press Event Agenda and News ReleaseABC6/FOX28No ratings yet
- Data Mei FinishDocument39 pagesData Mei FinishNi Putu Ari FebriantariNo ratings yet