You might also like
- Pharmacology Review For NursesDocument11 pagesPharmacology Review For Nursesisabel_avancena100% (4)
- Nursing Pharmacology Handouts For ZamboDocument7 pagesNursing Pharmacology Handouts For ZamboAlexa Abidin Oldenborg100% (8)
- PharmacologyDocument33 pagesPharmacologyFreeNursingNotes90% (67)
- Pharmacology HESI Review: Drugs Affecting the Nervous System and Cardiovascular SystemDocument13 pagesPharmacology HESI Review: Drugs Affecting the Nervous System and Cardiovascular Systemhkw0006164% (11)
- Nursing PharmacologyDocument22 pagesNursing PharmacologyDharren Rojan Garvida Agullana100% (2)
- Pharmacology Reviewer #01Document21 pagesPharmacology Reviewer #01Cutie Patootie100% (1)
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
- PharmacologyDocument21 pagesPharmacologyMaridel Estioco100% (3)
- Nursing Pharmacology COMPLETEDocument40 pagesNursing Pharmacology COMPLETEMonique Leonardo100% (8)
- Nclex Cram SheetDocument24 pagesNclex Cram Sheettoni100% (4)
- Pharmacology Study Guide For NursingDocument12 pagesPharmacology Study Guide For Nursingmadison61404100% (7)
- Pharmacology Notes NursingDocument25 pagesPharmacology Notes NursingKyle Marks100% (5)
- Pharmacology Nursing ReviewDocument19 pagesPharmacology Nursing Reviewp_dawg50% (2)
- Review Notes in Pharmacology - NCLEXDocument1 pageReview Notes in Pharmacology - NCLEXLalaine April E. Ortiola79% (29)
- PharmacologyDocument10 pagesPharmacologyPrince Mark Badillo100% (2)
- PHARMACOLOGY MNEMONICS: 38 CHARACTER TITLEDocument24 pagesPHARMACOLOGY MNEMONICS: 38 CHARACTER TITLEMrs3carpediem0% (1)
- Pharm ATIDocument5 pagesPharm ATIJennifer Vicioso86% (7)
- Pharmacology Nursing FinalDocument3 pagesPharmacology Nursing Finalrobinkirven100% (1)
- NURSING PHARMACOLOGY TIPSDocument19 pagesNURSING PHARMACOLOGY TIPSmaniz442100% (2)
- Drug Charts: Pharmacology OverviewDocument39 pagesDrug Charts: Pharmacology OverviewAsim Ishaq100% (5)
- Pharmacology ReviewDocument28 pagesPharmacology ReviewKathy Wollschleger100% (1)
- Nclex PharmaDocument22 pagesNclex Pharmakennedy14344No ratings yet
- Pharmacology SummaryDocument32 pagesPharmacology Summaryminikatiting95% (22)
- Pharmacology Nursing Flashcards Pinterest PinsDocument2 pagesPharmacology Nursing Flashcards Pinterest PinsSareeya Shre100% (1)
- Pharmacology SummaryDocument16 pagesPharmacology Summarysechzhen96% (46)
- Patho Physiology Bible: Over 70 Concept MapsDocument139 pagesPatho Physiology Bible: Over 70 Concept Mapslauramphs79100% (5)
- Hesi NR292 ESE Study GuideDocument16 pagesHesi NR292 ESE Study Guidenaijababy89100% (12)
- Pharmacology Study Notes - Adrenergic DrugsDocument2 pagesPharmacology Study Notes - Adrenergic Drugsstuckaluck83% (6)
- Pharmacology MnemonicsDocument17 pagesPharmacology MnemonicsJuvenis SampangNo ratings yet
- Drugs WorksheetDocument16 pagesDrugs Worksheetninja-2001No ratings yet
- Nursing PharmacologyDocument13 pagesNursing Pharmacologyjeshema100% (4)
- NCLEX Questions: 70Document17 pagesNCLEX Questions: 70RJ MarthewNo ratings yet
- Pharmacology Practice Test For NclexDocument10 pagesPharmacology Practice Test For NclexKira99% (96)
- Nursing School Drug ChartDocument13 pagesNursing School Drug ChartEve Lester100% (3)
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- Nursing Mnemonics: The Ultimate Tips and Notes For NursesFrom EverandNursing Mnemonics: The Ultimate Tips and Notes For NursesRating: 5 out of 5 stars5/5 (1)
- 140 Must Know Meds Demolish Nursing PharmacologyFrom Everand140 Must Know Meds Demolish Nursing PharmacologyRating: 4 out of 5 stars4/5 (18)
- Fluid and Electrolytes for Nursing StudentsFrom EverandFluid and Electrolytes for Nursing StudentsRating: 5 out of 5 stars5/5 (12)
- Fun with Pharmacology: Pharmacology Made SimpleFrom EverandFun with Pharmacology: Pharmacology Made SimpleRating: 3 out of 5 stars3/5 (1)
- Pharmacology BY: Hermie M. Pueyo M.D., R.N. PharmacologyDocument30 pagesPharmacology BY: Hermie M. Pueyo M.D., R.N. PharmacologyjessieNo ratings yet
- Pharmacology NotesDocument30 pagesPharmacology NotesJessica WalkerNo ratings yet
- Pharmacology Classifications and Administration TipsDocument16 pagesPharmacology Classifications and Administration TipsMary Roan RonatoNo ratings yet
- PharmaDocument20 pagesPharmaMary Roan RonatoNo ratings yet
- Pharmacology: By: Jan Michael Khalid L. Macarambon, RNDocument164 pagesPharmacology: By: Jan Michael Khalid L. Macarambon, RNJan MacarambonNo ratings yet
- PharmacologyDocument12 pagesPharmacologyXyra Linn InfanteNo ratings yet
- Pharmacology: By: Jan Michael Khalid L. Macarambon, RNDocument164 pagesPharmacology: By: Jan Michael Khalid L. Macarambon, RNJan MacarambonNo ratings yet
- Drug Book On EmergencyDocument21 pagesDrug Book On EmergencyDimpal Choudhary100% (3)
- Analgesics ContentDocument11 pagesAnalgesics ContentELISION OFFICIALNo ratings yet
- Analgesics Content (AutoRecovered)Document11 pagesAnalgesics Content (AutoRecovered)ELISION OFFICIALNo ratings yet
- Untitled Document PDFDocument3 pagesUntitled Document PDFdzmtz02No ratings yet
- Metronidazole drug information summaryDocument4 pagesMetronidazole drug information summaryKaloy AnneNo ratings yet
- Nursing Pharmacology HandoutsDocument10 pagesNursing Pharmacology HandoutsMICHAELA TIMBOLNo ratings yet
- Chapter 13 PharmacologyDocument35 pagesChapter 13 PharmacologyEdelrose LapitanNo ratings yet
- Drug Study ON Cabergolin EDocument4 pagesDrug Study ON Cabergolin ESimran SimzNo ratings yet
- P-Mid Midterm ExamDocument10 pagesP-Mid Midterm ExamIan Mizzel A. DulfinaNo ratings yet
- A (H1N1) Vaccine: Questions AnsweredDocument6 pagesA (H1N1) Vaccine: Questions Answeredjava_biscocho1229No ratings yet
- Professional Adjustment: A ReviewDocument41 pagesProfessional Adjustment: A Reviewjava_biscocho1229100% (3)
- Bronchial Asthma: A Case PresentationDocument59 pagesBronchial Asthma: A Case Presentationjava_biscocho122985% (39)
- NCP Pain1Document4 pagesNCP Pain1java_biscocho12290% (1)
- NCP-Ineffective AirwayDocument5 pagesNCP-Ineffective Airwayjava_biscocho1229No ratings yet
- ARTS: Aliswag Review and Training Specialists, IncDocument23 pagesARTS: Aliswag Review and Training Specialists, Incjava_biscocho1229No ratings yet
- Leprosy: A Case PresentationDocument36 pagesLeprosy: A Case Presentationjava_biscocho122970% (10)
- NCP-Effective Breast FeedingDocument3 pagesNCP-Effective Breast Feedingjava_biscocho12290% (1)
- History of Nursing-An OverviewDocument5 pagesHistory of Nursing-An Overviewjava_biscocho1229100% (3)
- Anatomy and Physiology-A ReviewDocument38 pagesAnatomy and Physiology-A Reviewjava_biscocho1229100% (4)
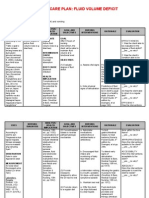
- NCP-Fluid Volume DeficitDocument2 pagesNCP-Fluid Volume Deficitjava_biscocho122979% (33)
- Nursing Abbreviations, Prefixes and SuffixesDocument10 pagesNursing Abbreviations, Prefixes and Suffixesjava_biscocho1229100% (4)
- OUR WORLD-North AmericaDocument46 pagesOUR WORLD-North Americajava_biscocho1229No ratings yet
- NCP Nutrition1Document4 pagesNCP Nutrition1java_biscocho1229100% (1)
- Integrated Management of Childhood IllnessDocument83 pagesIntegrated Management of Childhood Illnessjava_biscocho1229No ratings yet
- Eucharistic CelebrationDocument40 pagesEucharistic Celebrationjava_biscocho12290% (1)
- Leopold' ManeuversDocument3 pagesLeopold' Maneuversjava_biscocho122995% (22)
- Nursing Theories and Conceptual FrameworkDocument3 pagesNursing Theories and Conceptual Frameworkjava_biscocho1229100% (3)
- Herbal Medicines in The PhilippinesDocument20 pagesHerbal Medicines in The Philippinesjava_biscocho122997% (33)
- Reviewer - Life of Dr. Jose RizalDocument35 pagesReviewer - Life of Dr. Jose Rizaljava_biscocho122993% (105)
- Nursing Core Competencies For Quality LevelDocument5 pagesNursing Core Competencies For Quality Leveljava_biscocho1229No ratings yet
- The Language of AnatomyDocument4 pagesThe Language of Anatomyjava_biscocho122950% (2)
- TunnelDocument2 pagesTunneljava_biscocho1229No ratings yet
- As A Future NurseDocument1 pageAs A Future Nursejava_biscocho1229No ratings yet
- Mental Defense MechanismsDocument2 pagesMental Defense Mechanismsjava_biscocho1229100% (2)
- Water and Landforms in The PhilippinesDocument15 pagesWater and Landforms in The Philippinesjava_biscocho122988% (48)
- Antasida, Ah2, SitoprotektorDocument48 pagesAntasida, Ah2, SitoprotektorYulia KasihNo ratings yet
- Fluvoxamine MaleateDocument3 pagesFluvoxamine MaleateHilman Fitriaji Suganda PrawiraNo ratings yet
- Reviewer PcolDocument3 pagesReviewer PcolMycaela Archivido De AlvaNo ratings yet
- What You Should Know About Roactemra Safety BrochureDocument9 pagesWhat You Should Know About Roactemra Safety Brochureftzo3439No ratings yet
- 3911 Human EnUserGuide Neurobion 1.3.3.2 English LeafletDocument1 page3911 Human EnUserGuide Neurobion 1.3.3.2 English LeafletNadia AfifahNo ratings yet
- Dangerous drug prescription errorsDocument2 pagesDangerous drug prescription errorsCASSEY ANNE LARANo ratings yet
- ANXIETYDocument6 pagesANXIETYchirimallaNo ratings yet
- 6 SyrupsDocument37 pages6 Syrups鄭宇揚No ratings yet
- Obat PatenDocument8 pagesObat PatenrismaNo ratings yet
- Pakistan Pharma Industry SWOT AnalysisDocument7 pagesPakistan Pharma Industry SWOT AnalysisMehr SaqibNo ratings yet
- Drug treatments for coughDocument28 pagesDrug treatments for coughShaan Rules100% (1)
- Anger ManagementDocument3 pagesAnger ManagementMarina IvanNo ratings yet
- Acetaminophen Properties Clinical Uses and Adverse Effects PDFDocument218 pagesAcetaminophen Properties Clinical Uses and Adverse Effects PDFmirza_baig_46No ratings yet
- Naloxone in AdultsDocument8 pagesNaloxone in AdultsRoboschi StefaniaNo ratings yet
- Jurnal Hipertiroid KehamilanDocument5 pagesJurnal Hipertiroid KehamilanAbdurrohman IzzuddinNo ratings yet
- Medication Safety Incident Report Form Pharmacy Error EFormDocument3 pagesMedication Safety Incident Report Form Pharmacy Error EFormDauzheva Bro100% (1)
- Drug Abuse Screening Test 105 PDFDocument2 pagesDrug Abuse Screening Test 105 PDFAnand KirtiNo ratings yet
- NCPDocument5 pagesNCPCJ AngelesNo ratings yet
- Actos Avandia AWP PDFDocument11 pagesActos Avandia AWP PDFbmartindoyle6396No ratings yet
- 2008 Drug Trend ReportDocument108 pages2008 Drug Trend Report阿龟100% (2)
- Plymouth Hospitals Guide to Nasogastric and Gastrostomy FeedingDocument45 pagesPlymouth Hospitals Guide to Nasogastric and Gastrostomy FeedingbandarascbNo ratings yet
- PSR-0082: Proliferation of Internationally and Locally Manufactured Falsified MedicinesDocument2 pagesPSR-0082: Proliferation of Internationally and Locally Manufactured Falsified MedicinesRalph RectoNo ratings yet
- NCCN Guidelines Antiemesis v1.2017Document61 pagesNCCN Guidelines Antiemesis v1.2017Verneck SilvaNo ratings yet
- STIMULI To The REVISION PROCESS An Evaluation of The Indifference Zone of The USP 905 Content Uniformity Test1Document21 pagesSTIMULI To The REVISION PROCESS An Evaluation of The Indifference Zone of The USP 905 Content Uniformity Test1jljimenez1969No ratings yet
- Chemotherapy DrugsDocument5 pagesChemotherapy DrugsvmanuNo ratings yet
- ThyroidectomyDocument4 pagesThyroidectomyHSEINNo ratings yet
- Prescription Drug Abuse in Los Angeles County: Background and Recommendations For ActionDocument20 pagesPrescription Drug Abuse in Los Angeles County: Background and Recommendations For ActionSouthern California Public RadioNo ratings yet
- 2011 Call App - in Re CC - FB Evid in Custody CaseDocument12 pages2011 Call App - in Re CC - FB Evid in Custody CaseBrian WassomNo ratings yet
- Uniformity Dosage Unit USPDocument4 pagesUniformity Dosage Unit USPwike marelitaNo ratings yet
- Handin 1 - Cialis PPT PresentationDocument14 pagesHandin 1 - Cialis PPT PresentationMia_NaterNo ratings yet