You might also like
- Dampak Jangka Panjang StuntingDocument37 pagesDampak Jangka Panjang StuntingFina GisnawatyNo ratings yet
- Infant and Child Nutrition: Key PointsDocument4 pagesInfant and Child Nutrition: Key PointsseptiNo ratings yet
- Revised PPT Obesitas Anak FitriaDocument22 pagesRevised PPT Obesitas Anak FitriaFitri RahmawatiNo ratings yet
- Fluid Managementuntuk Mahasiswa SajaDocument56 pagesFluid Managementuntuk Mahasiswa SajaPratami Rieuwpassa IINo ratings yet
- Support Feeding - Tugas Mata Kuliah Nutrisi Klinis - Annisa FathadinaDocument66 pagesSupport Feeding - Tugas Mata Kuliah Nutrisi Klinis - Annisa FathadinaAnnisa FathadinaNo ratings yet
- Kasus Gastro (2020!07!23) Right Cardiac Failure Due To Right Atrium and Inferior Vena Cava Thrombus Tumor Related To HCCDocument32 pagesKasus Gastro (2020!07!23) Right Cardiac Failure Due To Right Atrium and Inferior Vena Cava Thrombus Tumor Related To HCCMukhammadBurhanuddinNo ratings yet
- Interpretasi GrowthchartDocument4 pagesInterpretasi GrowthchartHeri Hrisikesa WjgNo ratings yet
- Centile ChartsDocument20 pagesCentile ChartsJames DaviesNo ratings yet
- Ilmu Gizi Manusia Solo 2019Document53 pagesIlmu Gizi Manusia Solo 2019Roni NurdiantoNo ratings yet
- Implication of Parenteral NutritionDocument78 pagesImplication of Parenteral NutritionekoNo ratings yet
- Enteral Nutrition of Preterm BabyDocument54 pagesEnteral Nutrition of Preterm Babylordoftheweb100% (5)
- Obesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Document27 pagesObesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Andrie WigunaNo ratings yet
- Growth Charts WHO & IAPDocument63 pagesGrowth Charts WHO & IAPGovindan MayavanNo ratings yet
- Girls Growth Chart Well Child A4Document2 pagesGirls Growth Chart Well Child A4Devin FarmeryNo ratings yet
- Faltering Growth: Straight To The Point of CareDocument35 pagesFaltering Growth: Straight To The Point of Careftah ahmedNo ratings yet
- Parental Height and Stunting: 15 National Congress of Indonesian Nutrition Association Yogyakarta, IndonesiaDocument24 pagesParental Height and Stunting: 15 National Congress of Indonesian Nutrition Association Yogyakarta, Indonesiaputri annikeNo ratings yet
- MalariaDocument23 pagesMalariaIBhe Damianry QritezzNo ratings yet
- Referat ObesitasDocument20 pagesReferat ObesitasfaisalNo ratings yet
- Ventilasi Mekanik Untuk Neonatus: Dr. R. Adhi Teguh Perma Iskandar Sp.A Divisi Perinatologi FKUI-RSCMDocument52 pagesVentilasi Mekanik Untuk Neonatus: Dr. R. Adhi Teguh Perma Iskandar Sp.A Divisi Perinatologi FKUI-RSCMireneaureliaNo ratings yet
- 15th Indonesian Congress of PediatricsDocument52 pages15th Indonesian Congress of PediatricsDody FirmandaNo ratings yet
- Kuliah Pengayaan DM 2017-1Document100 pagesKuliah Pengayaan DM 2017-1Syarifah Maharani HidayatNo ratings yet
- MVDBWP VP ZL UP3 L 4 V5 XH G1636761573Document23 pagesMVDBWP VP ZL UP3 L 4 V5 XH G1636761573Ummu muzhaffarNo ratings yet
- Effect of Ursodeoxycholic Acid On Indirect Hyperbilirubinemia in Neonates Treated With PhototherapyDocument4 pagesEffect of Ursodeoxycholic Acid On Indirect Hyperbilirubinemia in Neonates Treated With PhototherapyEka Satria AnanditaNo ratings yet
- WHO 2009 Dengue ClassificationDocument31 pagesWHO 2009 Dengue ClassificationGarata DwiNo ratings yet
- Fluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversityDocument61 pagesFluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversitygozaNo ratings yet
- Subang Stunting 29 Juli 2019Document39 pagesSubang Stunting 29 Juli 2019Dika Andrian NugrahaNo ratings yet
- DR Arun Aggarwal Gastroenterologist: - Total Parenteral NutritionDocument37 pagesDR Arun Aggarwal Gastroenterologist: - Total Parenteral NutritionDr. Arun Aggarwal GastroenterologistNo ratings yet
- Feeding The Preterm-ConsensusDocument124 pagesFeeding The Preterm-ConsensusJuan Diego Lázaro TorresNo ratings yet
- Rekapitulasi Nilai PPDS IKA FK USU RMSDocument54 pagesRekapitulasi Nilai PPDS IKA FK USU RMSRizal Marubob SilalahiNo ratings yet
- Diet Iron AvidityDocument1 pageDiet Iron AvidityEnziana MaharaniNo ratings yet
- Pemantauan Bayi Prematur (Revisi)Document33 pagesPemantauan Bayi Prematur (Revisi)nur_betaNo ratings yet
- Japanese EncephalitisDocument14 pagesJapanese EncephalitisMuhammad Rafli AkbarNo ratings yet
- Wsop Asma - Prof Bambang SDocument67 pagesWsop Asma - Prof Bambang SSiti Arieanni KesumaNo ratings yet
- 1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018Document46 pages1-Fluid Management in Critically Ill Patients - Update Int Med Feb2018ดนุ เกษรศิริNo ratings yet
- Introduction - Prof SudigdoDocument49 pagesIntroduction - Prof Sudigdoyulia fatma nstNo ratings yet
- Prokab 6, ASRAWATI Tampil PDFDocument44 pagesProkab 6, ASRAWATI Tampil PDFNiceFenobileri OnFireNo ratings yet
- 3rd Nutrimet 2019 PROCEEDING BOOK PDFDocument82 pages3rd Nutrimet 2019 PROCEEDING BOOK PDFPutri NasutionNo ratings yet
- Ilmu Kesehatan Anak: Judul Materi: Pendekatan Anemia Pada AnakDocument103 pagesIlmu Kesehatan Anak: Judul Materi: Pendekatan Anemia Pada AnakDhanin WitedjaNo ratings yet
- Yes, Materi 16 Januari 2013Document42 pagesYes, Materi 16 Januari 2013Hendra SetyawanNo ratings yet
- Obesity in ChildrenDocument15 pagesObesity in ChildrenJohn ConnorNo ratings yet
- Strategi Penanganan Gangguan (Speech Delay) Terhadap Interaksi Sosial Anak Usia Dini Di TK Negeri Pembina SurabayaDocument14 pagesStrategi Penanganan Gangguan (Speech Delay) Terhadap Interaksi Sosial Anak Usia Dini Di TK Negeri Pembina SurabayaRosida WatiNo ratings yet
- Samsulhadi. Dept. of Obstetric & Gynecology, Fac. of Medicine Airlangga University. Dr. Soetomo Hospital Surabaya 26 MEI 2012Document87 pagesSamsulhadi. Dept. of Obstetric & Gynecology, Fac. of Medicine Airlangga University. Dr. Soetomo Hospital Surabaya 26 MEI 2012vera anastasyaNo ratings yet
- Sindroma Metabolik Dislipidemia Dan ObesitasDocument45 pagesSindroma Metabolik Dislipidemia Dan ObesitasLaurentius Juan WicaksonoNo ratings yet
- Childhood ObesityDocument70 pagesChildhood ObesityMedical SuperintendentNo ratings yet
- Weight Velocity Girls 3mon PDocument1 pageWeight Velocity Girls 3mon PdhikaNo ratings yet
- Diagnostic Approach of Short Stature / Stunted (Jan 2015) - Prof DR Jose BatubaraDocument49 pagesDiagnostic Approach of Short Stature / Stunted (Jan 2015) - Prof DR Jose BatubaraGerakan Kesehatan Ibu dan AnakNo ratings yet
- Sumber CPDocument9 pagesSumber CPArie RezaNo ratings yet
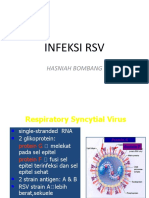
- Infeksi RSV: Hasniah BombangDocument12 pagesInfeksi RSV: Hasniah Bombangmuh hardiansyahNo ratings yet
- Newborn Screening PKB IDAI Papua DR - SandraDocument39 pagesNewborn Screening PKB IDAI Papua DR - SandraIBhe Damianry QritezzNo ratings yet
- BBLRDocument37 pagesBBLRHernina OktavianiNo ratings yet
- Child Health Problems GlobalDocument86 pagesChild Health Problems GlobalBagus P Agen SuplierNo ratings yet
- Who Reccomendation MalnutritionDocument123 pagesWho Reccomendation MalnutritionAgaipNo ratings yet
- Lembar Jawaban MCQ Nas 19 Okt 2017Document1 pageLembar Jawaban MCQ Nas 19 Okt 2017WirawanSiregarNo ratings yet
- Hamed2016Document4 pagesHamed2016Franknanda D'enzieroX-zhirawaxaveriuz PutrascreamoDark-nataseNo ratings yet
- Pediatric Normal ValueDocument4 pagesPediatric Normal ValueyaniarsusinNo ratings yet
- Stunting (EDIT)Document62 pagesStunting (EDIT)Eka RahmawatiNo ratings yet
- 1 Kuliah Pakar GD in Children ArianiDocument85 pages1 Kuliah Pakar GD in Children ArianiLendy Novaulia RosresNo ratings yet
- CDC 58669 DS1Document6 pagesCDC 58669 DS1Ngô Hoàng HuyNo ratings yet
- Chapter 1Document2 pagesChapter 1RC SectionNo ratings yet
- Letters: Trends in Obesity and Severe Obesity Prevalence in US Youth and Adults by Sex and Age, 2007-2008 To 2015-2016Document3 pagesLetters: Trends in Obesity and Severe Obesity Prevalence in US Youth and Adults by Sex and Age, 2007-2008 To 2015-2016Nouman Safdar AliNo ratings yet
- Stunting (EDIT)Document62 pagesStunting (EDIT)846035No ratings yet
- RJ45 To RJ11 CablingDocument7 pagesRJ45 To RJ11 CablingAyah Arya100% (1)
- Pemantauan Bayi Prematur (Revisi) PDFDocument33 pagesPemantauan Bayi Prematur (Revisi) PDF846035No ratings yet
- Tugas 1 Mekatan 2 T.O.CDocument5 pagesTugas 1 Mekatan 2 T.O.C846035No ratings yet
- Stunting (EDIT)Document62 pagesStunting (EDIT)846035No ratings yet
- Rabu, 20 Jul 2016Document32 pagesRabu, 20 Jul 2016nur_betaNo ratings yet
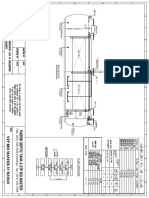
- Flow System Ipal 6.12.17Document1 pageFlow System Ipal 6.12.17846035No ratings yet
- Rabu, 20 Jul 2016Document32 pagesRabu, 20 Jul 2016nur_betaNo ratings yet
- Bblr-Ols 2015 (DR Aryono)Document52 pagesBblr-Ols 2015 (DR Aryono)846035No ratings yet
- I. 4 - Suku Cadang Kendaraan BermotorDocument3 pagesI. 4 - Suku Cadang Kendaraan BermotorMirna KristiyantoNo ratings yet
- Gambar DenahDocument3 pagesGambar Denah846035No ratings yet
- I. 5 - Alat-Alat ListrikDocument68 pagesI. 5 - Alat-Alat ListrikAgun GunawanNo ratings yet
- I. 5 - Alat-Alat ListrikDocument68 pagesI. 5 - Alat-Alat ListrikAgun GunawanNo ratings yet
- Oec-Covid-19-Guidance-For-Child-Care June 1Document25 pagesOec-Covid-19-Guidance-For-Child-Care June 1api-244363080No ratings yet
- Health and Wellness Women HealthDocument24 pagesHealth and Wellness Women HealthShimmering MoonNo ratings yet
- COVID-19 Epidemiology and Response: Group IV OCTOBER 24, 2020Document50 pagesCOVID-19 Epidemiology and Response: Group IV OCTOBER 24, 2020Lemlem ArgawNo ratings yet
- What Is Ovarian CancerDocument2 pagesWhat Is Ovarian CancerArianaNo ratings yet
- Second Covid-19 Vaccine Boosters, ExplainedDocument10 pagesSecond Covid-19 Vaccine Boosters, ExplainedsiesmannNo ratings yet
- Oet 4Document17 pagesOet 4Myrella Marie0% (1)
- Critical Control Points and Operational Prerequisite ProgramsDocument33 pagesCritical Control Points and Operational Prerequisite ProgramsqtrystNo ratings yet
- Airborne DeseasesDocument10 pagesAirborne DeseaseswinarsohNo ratings yet
- Socio 102 Lesson 6. Sexual Health and HygieneDocument23 pagesSocio 102 Lesson 6. Sexual Health and HygieneVivian giducosNo ratings yet
- Week 14 CD QUIZ 23Document2 pagesWeek 14 CD QUIZ 23tina santiagoNo ratings yet
- FHN - Nursing Care Plan Constipation)Document3 pagesFHN - Nursing Care Plan Constipation)blahniksNo ratings yet
- Jama Woo 2021 Oi 210106 1635192380.82276Document8 pagesJama Woo 2021 Oi 210106 1635192380.82276Melissa GuerreroNo ratings yet
- Narrative Report On National Hand Washing Day Celebration: Department of EducationDocument3 pagesNarrative Report On National Hand Washing Day Celebration: Department of Educationlelibeth curadaNo ratings yet
- Seminar On Issues of Maternal and Child BirthDocument22 pagesSeminar On Issues of Maternal and Child Birthkathyayani arraNo ratings yet
- How To Stay HealthyDocument2 pagesHow To Stay HealthyMissdiary Rahman100% (1)
- BNS Narrative Presentation 2022Document2 pagesBNS Narrative Presentation 2022Rafael Palma BlguNo ratings yet
- Apbhp WorksheetsDocument22 pagesApbhp WorksheetsCharlie Cotoner FalgueraNo ratings yet
- JM TB 62 Job Safety Analysis Eng 1Document2 pagesJM TB 62 Job Safety Analysis Eng 1James MathaiNo ratings yet
- The Art and Technique of Installing Pipes5Document3 pagesThe Art and Technique of Installing Pipes5Harris LeeNo ratings yet
- Problem PrioritizationDocument2 pagesProblem PrioritizationRegie GonzagaNo ratings yet
- High Risk PregnancyDocument5 pagesHigh Risk Pregnancygracie_greys5755No ratings yet
- CHN Famorca SummaryDocument137 pagesCHN Famorca SummaryMIKAELA DAVIDNo ratings yet
- PreTest Obstetrics & Gynecology, Fifteenth EditionDocument255 pagesPreTest Obstetrics & Gynecology, Fifteenth EditionDr. Faeba JosephNo ratings yet
- Third Quarter Learning Activity Sheet in English-Week 4Document4 pagesThird Quarter Learning Activity Sheet in English-Week 4Justine Leigh FloresNo ratings yet
- Jurnal Pengobatan Empiris Keratitis BakterialDocument16 pagesJurnal Pengobatan Empiris Keratitis BakterialimuhammadfahmiNo ratings yet
- The 9 Principles of ExerciseDocument13 pagesThe 9 Principles of ExercisegundadanNo ratings yet
- Corner R. Delos Reyes-Murillo Street, Barangay West, Candoni, Negros Occidental 6110Document2 pagesCorner R. Delos Reyes-Murillo Street, Barangay West, Candoni, Negros Occidental 6110JUmel PajarilloNo ratings yet
- Eapp q2 m1Document2 pagesEapp q2 m1Petal Kate CornelioNo ratings yet
- Madurai RoadDocument3 pagesMadurai RoadSiva NatNo ratings yet
- CHN-RLE Module 1 (Hand Washing)Document7 pagesCHN-RLE Module 1 (Hand Washing)Ems Rio BalNo ratings yet