You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
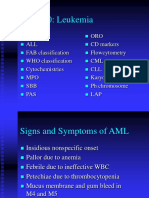
- LeukemiaDocument53 pagesLeukemiaAnnie GeorgeNo ratings yet
- JOB SUMMARY: To Plan, Organize and Implement An Appropriate NursingDocument2 pagesJOB SUMMARY: To Plan, Organize and Implement An Appropriate NursingAnnie GeorgeNo ratings yet
- Drug Presentation FormatDocument2 pagesDrug Presentation FormatAnnie GeorgeNo ratings yet
- Pediatric Review Questions - Mcqs I. Choose The Most Appropriate Answer and Write The Corresponding Alphabet in The Space ProvidedDocument2 pagesPediatric Review Questions - Mcqs I. Choose The Most Appropriate Answer and Write The Corresponding Alphabet in The Space ProvidedAnnie GeorgeNo ratings yet
- I Have A Friend WhoDocument1 pageI Have A Friend WhoAnnie GeorgeNo ratings yet
- Presentation of Communication and Professional Skills in EnglishDocument22 pagesPresentation of Communication and Professional Skills in EnglishAnnie GeorgeNo ratings yet
- The Art of Questioning: Annie Emerentia GeorgeDocument3 pagesThe Art of Questioning: Annie Emerentia GeorgeAnnie GeorgeNo ratings yet
- When Upon LifeDocument1 pageWhen Upon LifeAnnie GeorgeNo ratings yet
- Breast Tumors: Annie Emerentia GDocument8 pagesBreast Tumors: Annie Emerentia GAnnie GeorgeNo ratings yet
- Annie - Acid Base BalanceDocument34 pagesAnnie - Acid Base BalanceAnnie GeorgeNo ratings yet
- Carb Ho HydratesDocument24 pagesCarb Ho HydratesAnnie GeorgeNo ratings yet
- Lesson From A SparrowDocument2 pagesLesson From A SparrowAnnie GeorgeNo ratings yet
- Proteins - PPTX (Autosaved)Document31 pagesProteins - PPTX (Autosaved)Annie GeorgeNo ratings yet
- Guidelines For Entry and Exit From High Risk Areas - Infection ControlDocument19 pagesGuidelines For Entry and Exit From High Risk Areas - Infection ControlAnnie GeorgeNo ratings yet
- Preparation of Child For Diagnostic ProceduresDocument22 pagesPreparation of Child For Diagnostic ProceduresAnnie GeorgeNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Street Design Manual NYCDocument312 pagesStreet Design Manual NYCgonleoNo ratings yet
- C.E. 324 - Ethics - 1.0Document103 pagesC.E. 324 - Ethics - 1.0dela rosaNo ratings yet
- MHFU Hunter RankDocument5 pagesMHFU Hunter RankGustin PrayogoNo ratings yet
- Manuel Alava 01-12-10 PLDocument3 pagesManuel Alava 01-12-10 PLAshley RodriguezNo ratings yet
- Whirlpool Adg 789Document22 pagesWhirlpool Adg 789Laurentiu GramaNo ratings yet
- Anaerobic Degradation of Palm Oil Mill Ef Uent (POME)Document8 pagesAnaerobic Degradation of Palm Oil Mill Ef Uent (POME)HusainiNo ratings yet
- Pearson Correlation ValueDocument7 pagesPearson Correlation ValuemarianaNo ratings yet
- Dynamic Test Report of DECR-S Excitation Devices: ExperimenterDocument14 pagesDynamic Test Report of DECR-S Excitation Devices: ExperimenterSalmanEjazNo ratings yet
- Marcelo - GarciaDocument6 pagesMarcelo - GarciaNancy FernandezNo ratings yet
- WhittleMIME 413-513 Workshop 1 2014Document26 pagesWhittleMIME 413-513 Workshop 1 2014Diana Catalina Munera0% (1)
- Fact Sheeton Canola OilDocument15 pagesFact Sheeton Canola OilMonika ThadeaNo ratings yet
- YES-O Action-Plan - 2022-2023Document2 pagesYES-O Action-Plan - 2022-2023carmina duldulao100% (6)
- Aspen Tutorial #4: Design Specs & Sensitivity Analysis: OutlineDocument11 pagesAspen Tutorial #4: Design Specs & Sensitivity Analysis: OutlineWonda 005No ratings yet
- Who Has Allergies & Why: Allergies, Also Known As Allergic Diseases, Are A Number of Conditions Caused byDocument6 pagesWho Has Allergies & Why: Allergies, Also Known As Allergic Diseases, Are A Number of Conditions Caused byJun Dl CrzNo ratings yet
- Second Term English Exam: Level TCST June 2021Document6 pagesSecond Term English Exam: Level TCST June 2021benfaresNo ratings yet
- Listening DictationDocument3 pagesListening DictationThảo ĐinhNo ratings yet
- Power and Propulsion PDFDocument13 pagesPower and Propulsion PDFahmedalgaloNo ratings yet
- Yu-Gi-Oh GX Duel Academy - Written ExamDocument26 pagesYu-Gi-Oh GX Duel Academy - Written ExamisishamalielNo ratings yet
- B11 - Overload Relays (Ref) ENDocument20 pagesB11 - Overload Relays (Ref) ENAhmed AbazaNo ratings yet
- The Foods of Italy BookDocument92 pagesThe Foods of Italy BookmanupopNo ratings yet
- StringTokenizer in JavaDocument11 pagesStringTokenizer in JavaNeha saxena Neha saxenaNo ratings yet
- Economics 526 - Mathematics For Economists: Day(s) Time LocationDocument5 pagesEconomics 526 - Mathematics For Economists: Day(s) Time LocationGaurav JakhuNo ratings yet
- Full Site PDFDocument23 pagesFull Site PDFpursuwNo ratings yet
- Masterseal 530: Surface Applied Capillary Waterproofing For Concrete and MortarDocument2 pagesMasterseal 530: Surface Applied Capillary Waterproofing For Concrete and MortarHoang An ViNo ratings yet
- CPHL 214 Assignment 6Document2 pagesCPHL 214 Assignment 6NazNo ratings yet
- Fire AlarmDocument18 pagesFire AlarmgauriNo ratings yet
- Aljac Sampler: Environmentally Acceptable, Operationally Efficient and Safe, Eliminating Any Product LossDocument3 pagesAljac Sampler: Environmentally Acceptable, Operationally Efficient and Safe, Eliminating Any Product LossT. LimNo ratings yet
- Formula SheetDocument16 pagesFormula SheetgwerNo ratings yet
- Bleeding Disorders and Periodontology: P V & K PDocument13 pagesBleeding Disorders and Periodontology: P V & K PAdyas AdrianaNo ratings yet
- Video Wall, Digital Signage & C'Type Serial NumberDocument8 pagesVideo Wall, Digital Signage & C'Type Serial NumberAbhijit BarmanNo ratings yet