You might also like
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentFrom EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentNo ratings yet
- PyelonephritisDocument9 pagesPyelonephritisAfif Al FatihNo ratings yet
- Guide to Pediatric Urology and Surgery in Clinical PracticeFrom EverandGuide to Pediatric Urology and Surgery in Clinical PracticeNo ratings yet
- University of Al-Ameed / College of Medicine Department of PaediatricsDocument28 pagesUniversity of Al-Ameed / College of Medicine Department of Paediatricsاحمد الهاشميNo ratings yet
- UTIDocument46 pagesUTIKiran KommuNo ratings yet
- Infeccion Urinaria PCNA 2019Document13 pagesInfeccion Urinaria PCNA 2019andres felipe ramirezNo ratings yet
- DR - Mohaimen A.M Alkabi: University of Al-Ameed / College ofDocument28 pagesDR - Mohaimen A.M Alkabi: University of Al-Ameed / College ofاحمد الهاشميNo ratings yet
- Case Report Format 1Document23 pagesCase Report Format 1Nickaela CalalangNo ratings yet
- Pediatric Urinary DisordersDocument27 pagesPediatric Urinary DisordersKailash NagarNo ratings yet
- Uti 2Document3 pagesUti 2Jhoan de GuzmanNo ratings yet
- Aafp Uti GuidelinesDocument10 pagesAafp Uti GuidelinesCess Lagera YbanezNo ratings yet
- UTI (Urinary Tract Infection)Document9 pagesUTI (Urinary Tract Infection)Carson BirthNo ratings yet
- Healthmed 15 1 Evlijana ZulicDocument7 pagesHealthmed 15 1 Evlijana ZulicEdoHNo ratings yet
- Clinical Guideline For Childhood Urinary Tract Infection (Second Revision)Document9 pagesClinical Guideline For Childhood Urinary Tract Infection (Second Revision)joeunisaNo ratings yet
- Urinary Tract Infections: by John MbawaDocument33 pagesUrinary Tract Infections: by John MbawaAlvin OmondiNo ratings yet
- Urinary Tract Infections in Pregnancy: BackgroundDocument18 pagesUrinary Tract Infections in Pregnancy: BackgroundAqeel AhmedNo ratings yet
- Urinary Track Infection (Uti)Document8 pagesUrinary Track Infection (Uti)Praise ToluwalaseNo ratings yet
- Nelson IskDocument6 pagesNelson IskDellNo ratings yet
- Urinary Tract Infection FinalllllllllDocument55 pagesUrinary Tract Infection FinalllllllllBinita ShakyaNo ratings yet
- 8 Day Urinary Tract InfectionDocument9 pages8 Day Urinary Tract InfectionShreyash HaritwalNo ratings yet
- A Urinary Tract InfectionDocument5 pagesA Urinary Tract InfectionSushma ReddyNo ratings yet
- Urinary Tract Infections د.أحمد الأهنوميDocument44 pagesUrinary Tract Infections د.أحمد الأهنوميMohammad BelbahaithNo ratings yet
- Urinary Tract Infection in ChildrenDocument38 pagesUrinary Tract Infection in ChildrensivaNo ratings yet
- PyelonephritisDocument32 pagesPyelonephritisgeorgia.lang67% (3)
- Neonatal Hepatitis SyndromeDocument18 pagesNeonatal Hepatitis Syndromeenny_rommyNo ratings yet
- Uti ReadingsDocument6 pagesUti ReadingskarenbelnasNo ratings yet
- UTI - Internship PresentationDocument27 pagesUTI - Internship PresentationPernel Jose Alam MicuboNo ratings yet
- Case ManagementDocument11 pagesCase ManagementGabrielle CatalanNo ratings yet
- Urinary Tract Infection - A Suitable Approach: Lecture NotesDocument7 pagesUrinary Tract Infection - A Suitable Approach: Lecture NotesMary Hedweg OpenianoNo ratings yet
- UTI GuidelinesDocument7 pagesUTI GuidelinesstarkNo ratings yet
- Urinary Tract Infection: CC Ricky G. JalecoDocument56 pagesUrinary Tract Infection: CC Ricky G. JalecoRicky JalecoNo ratings yet
- Urinecollectionmethodsin Children:: Which Is The Best?Document7 pagesUrinecollectionmethodsin Children:: Which Is The Best?endah dwi cahyaniNo ratings yet
- Prune Belly SyndromeDocument39 pagesPrune Belly SyndromeHudaNo ratings yet
- UTI in Pregnancy - 071923Document14 pagesUTI in Pregnancy - 071923allanfocus91No ratings yet
- 8 Urinary Tract InfectionDocument4 pages8 Urinary Tract Infectionzainabd1964No ratings yet
- Utis in Pregnancy: Rachael Mweigwa NakimuliDocument55 pagesUtis in Pregnancy: Rachael Mweigwa NakimuliRuva Oscass JimmyNo ratings yet
- Help Pedsurgeryafrica80Document4 pagesHelp Pedsurgeryafrica80Thayalan SukumaranNo ratings yet
- Referat UtiDocument20 pagesReferat UtiYeni Rosa SitohangNo ratings yet
- Vesicoureteral RefluxDocument5 pagesVesicoureteral RefluxHUSAMNo ratings yet
- Urinary Tract InfectionsDocument6 pagesUrinary Tract Infectionspat_tienmin4552No ratings yet
- Pa Tho PhysiologyDocument2 pagesPa Tho PhysiologyKLaudine Mae Flores ÖNo ratings yet
- Child JournalDocument8 pagesChild JournalVijayakanth VijayakumarNo ratings yet
- Urinalysis (Ua) and The Diagnosis of UtisDocument5 pagesUrinalysis (Ua) and The Diagnosis of UtisErawati ArmayaniNo ratings yet
- UTI in DM - Super PaperDocument6 pagesUTI in DM - Super PaperLourdes Fernandez CabreraNo ratings yet
- Urinary Tract Infection in ChildrenDocument45 pagesUrinary Tract Infection in ChildrenMuhammad HaziqNo ratings yet
- Journal Reading UTIDocument25 pagesJournal Reading UTIBourbon ZeroNo ratings yet
- Infection Urinaire 2019Document11 pagesInfection Urinaire 2019KhaoulapediatreNo ratings yet
- Evaluation and Management UTI in Emergency-1-10Document10 pagesEvaluation and Management UTI in Emergency-1-10Ade PrawiraNo ratings yet
- Urinary Tract InfectionDocument10 pagesUrinary Tract InfectionditaNo ratings yet
- 1 s2.0 S0302283814011816 Main PDFDocument13 pages1 s2.0 S0302283814011816 Main PDFFahrizal Kusuma WNo ratings yet
- Stein R Et Al Paediatric Infections EUR UROL 67 2015 546 558 14826Document13 pagesStein R Et Al Paediatric Infections EUR UROL 67 2015 546 558 14826Olga CîrsteaNo ratings yet
- Uti Case StudyDocument7 pagesUti Case StudyStephNo ratings yet
- Urinary Tract Infections in ChildrenDocument22 pagesUrinary Tract Infections in Childrenmelese woldehawariatNo ratings yet
- Clinical Overview IvuDocument45 pagesClinical Overview IvularevalomunozNo ratings yet
- Uti PediaDocument8 pagesUti PediaNeenya SisonNo ratings yet
- CaseDocument7 pagesCaseTroy MirandaNo ratings yet
- Bacterial Uropathogenic FactorsDocument7 pagesBacterial Uropathogenic FactorsAtma AdiatmaNo ratings yet
- Uti 1Document75 pagesUti 1Muwanga faizoNo ratings yet
- K10 - ISK AtasDocument39 pagesK10 - ISK AtasfelixNo ratings yet
- Pediatric Urinary Tract Infection: Aprianda Saputra/ANSDocument34 pagesPediatric Urinary Tract Infection: Aprianda Saputra/ANSAkbar DarajatNo ratings yet
- 6 Thrombocytopenia-Min PDFDocument43 pages6 Thrombocytopenia-Min PDFyogeshraval368No ratings yet
- 3 Which Inotrops and When in NICU-min PDFDocument22 pages3 Which Inotrops and When in NICU-min PDFyogeshraval368No ratings yet
- Guideline Management of Congenital Heart Diseases: ObjectivesDocument43 pagesGuideline Management of Congenital Heart Diseases: Objectivesyogeshraval368No ratings yet
- Accidental ExtubationDocument3 pagesAccidental Extubationyogeshraval368No ratings yet
- Neonatal LupusDocument19 pagesNeonatal Lupusyogeshraval368No ratings yet
- WHO - Guidelines On Establishment of Virology LaboratoryDocument79 pagesWHO - Guidelines On Establishment of Virology LaboratoryAjeng MutvakadwiaNo ratings yet
- 3-2 MicrobiologicalQualityControlDocument37 pages3-2 MicrobiologicalQualityControlNuzul DianperdanaNo ratings yet
- Gram Negative Cocci-Sem 1.Document21 pagesGram Negative Cocci-Sem 1.Charmaine Corpuz GranilNo ratings yet
- Dengue DOHDocument16 pagesDengue DOHGehlatin Tumanan100% (1)
- Dental PlaqueDocument93 pagesDental Plaquebhasalepooja100% (1)
- CHN Pnle Board Exam Practice-Part 5Document6 pagesCHN Pnle Board Exam Practice-Part 5jerarddaria.elakNo ratings yet
- Antimicrobial Sensitivity TestingDocument21 pagesAntimicrobial Sensitivity TestingLaiba FarooqNo ratings yet
- Clinical Microbiology QuestionsDocument18 pagesClinical Microbiology QuestionsArianne Joy C. TamarayNo ratings yet
- Sample Chapter IIDocument16 pagesSample Chapter IIKean CardenasNo ratings yet
- Dapus FixDocument2 pagesDapus FixIkrima MuhdarmuhallyNo ratings yet
- Anais (Hari)Document220 pagesAnais (Hari)kamalaziziNo ratings yet
- Information Sheet For CandidateDocument3 pagesInformation Sheet For CandidatejljoioiuNo ratings yet
- Food PoisoningDocument55 pagesFood PoisoningAnusikta PandaNo ratings yet
- Feline Panleukopenia Virus Infection and Other Viral EnteritidesDocument8 pagesFeline Panleukopenia Virus Infection and Other Viral EnteritidesjohanNo ratings yet
- MCQs in para (With Answers)Document20 pagesMCQs in para (With Answers)janiceli020785% (26)
- Rohela Mahmud, Yvonne Ai Lian Lim, Amirah Amir - Medical Parasitology - A Textbook (2017, Springer International Publishing)Document198 pagesRohela Mahmud, Yvonne Ai Lian Lim, Amirah Amir - Medical Parasitology - A Textbook (2017, Springer International Publishing)Brant100% (2)
- Infección VIH Primer 2023Document21 pagesInfección VIH Primer 2023MedicazoNo ratings yet
- Diphtheria, Enterobiasis, FilariasisDocument2 pagesDiphtheria, Enterobiasis, FilariasisAngel Joy CatalanNo ratings yet
- Materi DR DR Ari Prayitno SpAK Typhoid Vaccine - Current and New PlatformDocument40 pagesMateri DR DR Ari Prayitno SpAK Typhoid Vaccine - Current and New PlatformMutiara UtiNo ratings yet
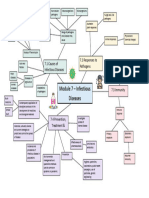
- Module 7 Mind Map BiologyDocument1 pageModule 7 Mind Map BiologyAltSpace TimeNo ratings yet
- Acute and Chronic PharyngitisDocument10 pagesAcute and Chronic PharyngitisUjjawalShriwastavNo ratings yet
- MIC 211 Prac 4 DiscussionDocument2 pagesMIC 211 Prac 4 Discussionmnukwa wendieNo ratings yet
- MicrobiologyDocument675 pagesMicrobiologyzakarya alamamiNo ratings yet
- Leptospirosis UPH 2Document33 pagesLeptospirosis UPH 2Joshua ObrienNo ratings yet
- Pneumonia PresentationDocument23 pagesPneumonia Presentationapi-546694141No ratings yet
- Vis Rabies PDFDocument2 pagesVis Rabies PDFFA AnthonyNo ratings yet
- Ams Ipc SlidesDocument36 pagesAms Ipc SlidesHarriet TembaNo ratings yet
- Interpretation: S16 - Mrs - Bina FPSC 21-D (Faridabad)Document2 pagesInterpretation: S16 - Mrs - Bina FPSC 21-D (Faridabad)Deepak JainNo ratings yet
- Lab 3 HandlingDocument11 pagesLab 3 HandlingAAANo ratings yet
- Intro BacteriaDocument47 pagesIntro BacteriaMj BrionesNo ratings yet