You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Blood Pressure Solution Ebook 022318Document14 pagesThe Blood Pressure Solution Ebook 022318Rolando M Tabora100% (2)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- First AidDocument1,202 pagesFirst AidAnonymous QVovunM100% (17)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Basic ECG Interpretation MWDocument211 pagesBasic ECG Interpretation MWLorelie AsisNo ratings yet
- 1 Practise Questions Keith Moore 5th Edition Should ReadDocument113 pages1 Practise Questions Keith Moore 5th Edition Should ReadNasan Shehada100% (1)
- Lewis: Medical-Surgical Nursing, 8 Edition: Chapter 36: Nursing Management: Dysrhythmias Key Points - PrintableDocument6 pagesLewis: Medical-Surgical Nursing, 8 Edition: Chapter 36: Nursing Management: Dysrhythmias Key Points - PrintableMonica100% (1)
- Autopsy Report of Jim McDougalDocument11 pagesAutopsy Report of Jim McDougalBatmanrobin Robinbatman100% (2)
- Faisalabad Institute of Cardiology, Faisalabad.: Discharge SlipDocument1 pageFaisalabad Institute of Cardiology, Faisalabad.: Discharge SlipFarhanNo ratings yet
- Jaundice Case PrresentationDocument30 pagesJaundice Case PrresentationUday KumarNo ratings yet
- Newton Fund Institutional Links Grants - Application (2018 IL7 - April)Document31 pagesNewton Fund Institutional Links Grants - Application (2018 IL7 - April)Marzuki Panji WijayaNo ratings yet
- Venous Function and Central Venous Pressure: A Physiologic StoryDocument14 pagesVenous Function and Central Venous Pressure: A Physiologic StoryMarzuki Panji WijayaNo ratings yet
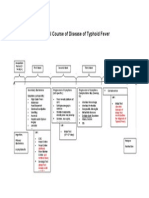
- Natural Course of Disease of Typhoid FeverDocument1 pageNatural Course of Disease of Typhoid FeverMarzuki Panji WijayaNo ratings yet
- Diabetes Education BookletDocument11 pagesDiabetes Education BookletMarzuki Panji WijayaNo ratings yet
- Diabetes Education BookletDocument11 pagesDiabetes Education BookletMarzuki Panji WijayaNo ratings yet
- Shock and Its Nursing InterventionsDocument3 pagesShock and Its Nursing InterventionsWendy EscalanteNo ratings yet
- CPRDocument18 pagesCPRSwamy MmsNo ratings yet
- Ncert Science NotesDocument75 pagesNcert Science NotesRobin SharmaNo ratings yet
- IGCSE BioDocument5 pagesIGCSE BioMajid DardasNo ratings yet
- Development of Cardiovascular SystemDocument8 pagesDevelopment of Cardiovascular Systemwmdpr4x64fNo ratings yet
- Frog Ncert Based QuestionsDocument7 pagesFrog Ncert Based Questionssrivaishna123100% (1)
- Princess Solmeron - Lesson 2 & 3Document15 pagesPrincess Solmeron - Lesson 2 & 3Princess Aliah SolmeronNo ratings yet
- ACS FianlDocument72 pagesACS FianlmawardikaNo ratings yet
- Planning Sports FacilitiesDocument41 pagesPlanning Sports FacilitiesMuhammad TariqNo ratings yet
- Drug Study AMIODARONE & PROPOFOLDocument3 pagesDrug Study AMIODARONE & PROPOFOLNIKKI CARYL ZAFRANo ratings yet
- Cath Lab - Interventional Radiology Nursing Skills ChecklistDocument7 pagesCath Lab - Interventional Radiology Nursing Skills Checklistdk15janNo ratings yet
- Congenital Abnormalities - WeziDocument192 pagesCongenital Abnormalities - WeziB & K GLUT FOODSNo ratings yet
- Professional Ethics and Responsibilities: Mitral ValveDocument9 pagesProfessional Ethics and Responsibilities: Mitral ValveMary LouNo ratings yet
- Jam's Final Papers in SaadDocument38 pagesJam's Final Papers in SaadMarinelle TumanguilNo ratings yet
- Unit 8Document34 pagesUnit 8Deta Meila PutriNo ratings yet
- Severe Hyperkalemia Can The Electrocardiogram Risk Stratify For Short-Term Adverse EventsDocument9 pagesSevere Hyperkalemia Can The Electrocardiogram Risk Stratify For Short-Term Adverse EventsCavalerul Mesei CromaticeNo ratings yet
- Acute Pulmonary Edema in PregnancyDocument20 pagesAcute Pulmonary Edema in PregnancyUtomo Budidarmo100% (1)
- Exchange Surfaces 1 QPDocument12 pagesExchange Surfaces 1 QPSaaleh AbanurNo ratings yet
- 2011-2012 Annual Report Department of Pediatrics Saint Louis University School of MedicineDocument131 pages2011-2012 Annual Report Department of Pediatrics Saint Louis University School of Medicineslusompeds0% (1)
- Biopotential Electrodes Class8 9Document30 pagesBiopotential Electrodes Class8 9ankushbrajNo ratings yet
- 6 Thrombosis MorphologyDocument20 pages6 Thrombosis MorphologySawera RaheemNo ratings yet
- Grade 11 Life Sciences Lesson PlansDocument31 pagesGrade 11 Life Sciences Lesson PlansDarlen May DalidaNo ratings yet