You might also like
- Role of Interleukin-6 in Ischemic Stroke OutcomeDocument7 pagesRole of Interleukin-6 in Ischemic Stroke OutcomeSalma SalmaNo ratings yet
- Articol BiochimieDocument6 pagesArticol BiochimieOti DeeaNo ratings yet
- Inflamation N StrokeDocument30 pagesInflamation N StrokeNona Suci rahayuNo ratings yet
- Encef Limbica 5Document10 pagesEncef Limbica 5Carolina MuñozNo ratings yet
- Stress Mediators and Immune Dysfunction in Patients With Acute Cerebrovascular DiseasesDocument10 pagesStress Mediators and Immune Dysfunction in Patients With Acute Cerebrovascular DiseasesBian Rahmadi MedikantoNo ratings yet
- Nejmc2008597 PDFDocument2 pagesNejmc2008597 PDFAdriana VasilicaNo ratings yet
- Fimmu 08 00112Document13 pagesFimmu 08 00112Sergeat18BNo ratings yet
- Dynamic Changes of - Melanocyte-Stimulating Hormone Levels in The Serum of Patients With Craniocerebral TraumaDocument6 pagesDynamic Changes of - Melanocyte-Stimulating Hormone Levels in The Serum of Patients With Craniocerebral TraumaAwilia Eka PutriNo ratings yet
- Bell 'S Palsy: Clinical and Neurophysiologic Predictors of RecoveryDocument5 pagesBell 'S Palsy: Clinical and Neurophysiologic Predictors of RecoveryMarsya Yulinesia LoppiesNo ratings yet
- Biomedicines 11 00044 v3Document19 pagesBiomedicines 11 00044 v3mariel gonzalezNo ratings yet
- 7 F 113 D-Vaxdeath Autopsy Comfirmed StudyDocument18 pages7 F 113 D-Vaxdeath Autopsy Comfirmed StudyropechainslingNo ratings yet
- HHS Public Access: Autoimmune EncephalopathiesDocument33 pagesHHS Public Access: Autoimmune EncephalopathiesLink BuiNo ratings yet
- Encefalitis AutoinmuneDocument8 pagesEncefalitis AutoinmuneRoosevelt Santibañez Dla TorreNo ratings yet
- Encefalitis AutoinmuneDocument18 pagesEncefalitis AutoinmunealmarazneurologiaNo ratings yet
- 6 Antithrombotic Therapy in Patients With Infective EndocarditisDocument12 pages6 Antithrombotic Therapy in Patients With Infective Endocarditisabdeali hazariNo ratings yet
- Encephalitis and Aseptic Meningitis: Short-Term and Long-Term Outcome, Quality of Life and Neuropsychological FunctioningDocument9 pagesEncephalitis and Aseptic Meningitis: Short-Term and Long-Term Outcome, Quality of Life and Neuropsychological FunctioningRoberto SoehartonoNo ratings yet
- Active and Passive Immunotherapy For Neurodegenerative DisordersDocument20 pagesActive and Passive Immunotherapy For Neurodegenerative DisordersDr rajaNo ratings yet
- Autoimmune Encephalitis Best PracticeDocument12 pagesAutoimmune Encephalitis Best PracticeKatrina San GilNo ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- Cei0121 0270Document5 pagesCei0121 0270Nur WahyuniNo ratings yet
- Autoimmune Encephalitis: Frequency and Prognosis: A. Al Ansari N. P. RobertsonDocument3 pagesAutoimmune Encephalitis: Frequency and Prognosis: A. Al Ansari N. P. RobertsonNathaly CantorNo ratings yet
- 2019 Autoimmune EncephalitidesDocument23 pages2019 Autoimmune EncephalitidesNeurologia homicNo ratings yet
- Armangue2014Document8 pagesArmangue2014etiyaNo ratings yet
- Neutrophil-To-Lymphocyte Ratio in Acute CerebralDocument9 pagesNeutrophil-To-Lymphocyte Ratio in Acute CerebralJorge Ramirez RaherNo ratings yet
- Diagnosis of Cerebral Toxoplasmosis in AIDS Patients in Brazil: Importance of Molecular and Immunological Methods Using Peripheral Blood SamplesDocument4 pagesDiagnosis of Cerebral Toxoplasmosis in AIDS Patients in Brazil: Importance of Molecular and Immunological Methods Using Peripheral Blood SamplesinezlithaNo ratings yet
- Stroke IskemikDocument7 pagesStroke IskemikMay MaghdalenaNo ratings yet
- Modelling Viral Encephalitis Caused by Herpes Simplex Virus 1 Infection in Cerebral OrganoidsDocument31 pagesModelling Viral Encephalitis Caused by Herpes Simplex Virus 1 Infection in Cerebral OrganoidsgugicevdzoceNo ratings yet
- 2021 Thrombocytopenia and Intracranial Venous Sinus Thrombosis AfterDocument10 pages2021 Thrombocytopenia and Intracranial Venous Sinus Thrombosis AfterBeatriz VásquezNo ratings yet
- Lattanzi2019 Article Neutrophil To LymphocyteRatioIDocument9 pagesLattanzi2019 Article Neutrophil To LymphocyteRatioISusanyi ErvinNo ratings yet
- Serum Biomarkers of Brain Injury After Uncomplicated Cardiac Surgery: Secondary Analysis From A Randomized TrialDocument7 pagesSerum Biomarkers of Brain Injury After Uncomplicated Cardiac Surgery: Secondary Analysis From A Randomized Trialjesus armando mandujano barcenasNo ratings yet
- B-Lymphocyte-Mediated Delayed Cognitive Impairment Following StrokeDocument13 pagesB-Lymphocyte-Mediated Delayed Cognitive Impairment Following Strokeasoly giovanoNo ratings yet
- Clinical Characteristics and PDocument10 pagesClinical Characteristics and Pmiss betawiNo ratings yet
- Activity IntrinsicDocument3 pagesActivity IntrinsicAna Tomas PetrovicNo ratings yet
- Neurorheumatology: A Comprehenisve Guide to Immune Mediated Disorders of the Nervous SystemFrom EverandNeurorheumatology: A Comprehenisve Guide to Immune Mediated Disorders of the Nervous SystemNo ratings yet
- Daniel PiriciDocument12 pagesDaniel PiriciRashellya RasyidaNo ratings yet
- Meningitis BacterialisDocument9 pagesMeningitis BacterialisReza OktaramaNo ratings yet
- Texto 2Document10 pagesTexto 2jjorge160570No ratings yet
- Encefaliti AutoimmuniDocument12 pagesEncefaliti AutoimmuniLallo CuluNo ratings yet
- Sdarticle 8Document6 pagesSdarticle 8Riddhi GandhiNo ratings yet
- Ehler201dd7 Article TranslationalEvidenceForTwoDisDocument10 pagesEhler201dd7 Article TranslationalEvidenceForTwoDisMark TomNo ratings yet
- Acn3 6 310Document14 pagesAcn3 6 310ErdaNo ratings yet
- Awad 290Document3 pagesAwad 290Sandra GuillenNo ratings yet
- Serum Markers of Brain Injury Can Predict Good Neurological Outcome After Out-Of-Hospital Cardiac ArrestDocument11 pagesSerum Markers of Brain Injury Can Predict Good Neurological Outcome After Out-Of-Hospital Cardiac ArrestIvan EzequielNo ratings yet
- Autoimmune EncephalitisDocument9 pagesAutoimmune Encephalitispiero reyesNo ratings yet
- Objetivo 3 Móvil PDFDocument26 pagesObjetivo 3 Móvil PDFnawal akarmaniNo ratings yet
- Molecular MimicryDocument15 pagesMolecular MimicryAshwinNo ratings yet
- Ambil PDF JTN 1966Document9 pagesAmbil PDF JTN 1966Naily Nuzulur RohmahNo ratings yet
- (10920684 - Neurosurgical Focus) The Role of ICP Monitoring in MeningitisDocument7 pages(10920684 - Neurosurgical Focus) The Role of ICP Monitoring in MeningitisLuqyani Trilandini MaryamNo ratings yet
- Seizures in Adults With Bacterial MeningitisDocument9 pagesSeizures in Adults With Bacterial MeningitiselaNo ratings yet
- Obling Et Al-2023-Intensive Care MedicineDocument12 pagesObling Et Al-2023-Intensive Care Medicinefatmaahmed3241No ratings yet
- 10.1515 - HSZ 2021 0413Document1 page10.1515 - HSZ 2021 0413xivydpndNo ratings yet
- REVISION jcm-2839576Document19 pagesREVISION jcm-2839576bibulkaNo ratings yet
- Case Report: Safety and Efficacy of Erythropoietin in Traumatic Brain Injury Patients: A Pilot Randomized TrialDocument5 pagesCase Report: Safety and Efficacy of Erythropoietin in Traumatic Brain Injury Patients: A Pilot Randomized TrialIqra AlghifarihNo ratings yet
- Autoimmunemeningitisand Encephalitis: Megan B. RichieDocument20 pagesAutoimmunemeningitisand Encephalitis: Megan B. RichieJuan Felipe Quintero MorenoNo ratings yet
- Ischemic Stroke A Comparative Retrospective Study: Experience of Military Hospital of MeknesDocument20 pagesIschemic Stroke A Comparative Retrospective Study: Experience of Military Hospital of MeknesIJAR JOURNALNo ratings yet
- High-Dose Corticosteroids After Spinal Cord Injury Reduce Neural Progenitor Cell ProliferationDocument11 pagesHigh-Dose Corticosteroids After Spinal Cord Injury Reduce Neural Progenitor Cell ProliferationVonalia Nurul AnnisaNo ratings yet
- Acute Disseminated Encephalomyelitis Post Sars-Cov-2 VaccinationDocument4 pagesAcute Disseminated Encephalomyelitis Post Sars-Cov-2 VaccinationIJAR JOURNALNo ratings yet
- Encefalite Autoimune Soronegativa - June 2023Document12 pagesEncefalite Autoimune Soronegativa - June 2023FernandoNo ratings yet
- Tosca 1996Document7 pagesTosca 1996HEARTJUGGLERNo ratings yet
- Diagnostic CriteriaDocument12 pagesDiagnostic CriteriaBenjamin NgNo ratings yet
- Bharti Airtel Strategy FinalDocument39 pagesBharti Airtel Strategy FinalniksforloveuNo ratings yet
- FIREBASE Edited PresentationDocument12 pagesFIREBASE Edited PresentationNiraj MirgalNo ratings yet
- A Project On "Automatic Water Sprinkler Based On Wet and Dry Conditions"Document28 pagesA Project On "Automatic Water Sprinkler Based On Wet and Dry Conditions"Srínívas SrínuNo ratings yet
- French Cuisine RecipeDocument6 pagesFrench Cuisine RecipeJimmy AchasNo ratings yet
- E-CRM Analytics The Role of Data Integra PDFDocument310 pagesE-CRM Analytics The Role of Data Integra PDFJohn JiménezNo ratings yet
- Lab Science of Materis ReportDocument22 pagesLab Science of Materis ReportKarl ToddNo ratings yet
- Quotation - 1Document4 pagesQuotation - 1haszirul ameerNo ratings yet
- Law of AttractionDocument2 pagesLaw of AttractionKate SummersNo ratings yet
- Acute Suppurative Otitis MediaDocument41 pagesAcute Suppurative Otitis Mediarani suwadjiNo ratings yet
- The Marriage of Figaro LibrettoDocument64 pagesThe Marriage of Figaro LibrettoTristan BartonNo ratings yet
- Canon I-SENSYS MF411dw Parts CatalogDocument79 pagesCanon I-SENSYS MF411dw Parts Catalogmarian100% (1)
- SCIENCE 11 WEEK 6c - Endogenic ProcessDocument57 pagesSCIENCE 11 WEEK 6c - Endogenic ProcessChristine CayosaNo ratings yet
- EC 2012 With SolutionsDocument50 pagesEC 2012 With Solutionsprabhjot singh1No ratings yet
- Req Equip Material Devlopment Power SectorDocument57 pagesReq Equip Material Devlopment Power Sectorayadav_196953No ratings yet
- CBSE 10th ResultsDocument1 pageCBSE 10th ResultsAkshit SinghNo ratings yet
- Post Renaissance Architecture in EuropeDocument10 pagesPost Renaissance Architecture in Europekali_007No ratings yet
- Landscape ArchitectureDocument9 pagesLandscape Architecturelisan2053No ratings yet
- Communicating Value - PatamilkaDocument12 pagesCommunicating Value - PatamilkaNeha ArumallaNo ratings yet
- Employee of The Month.Document2 pagesEmployee of The Month.munyekiNo ratings yet
- Documentos de ExportaçãoDocument17 pagesDocumentos de ExportaçãoZineNo ratings yet
- 2015 Student Handbook 16 January 2015Document66 pages2015 Student Handbook 16 January 2015John KhanNo ratings yet
- Affidavit of Co OwnershipDocument2 pagesAffidavit of Co OwnershipEmer MartinNo ratings yet
- Diagnosis ListDocument1 pageDiagnosis ListSenyorita KHayeNo ratings yet
- Wordbank 15 Coffee1Document2 pagesWordbank 15 Coffee1akbal13No ratings yet
- Financial Institutions Markets and ServicesDocument2 pagesFinancial Institutions Markets and ServicesPavneet Kaur Bhatia100% (1)
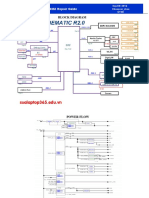
- Asus x453Document5 pagesAsus x453Rhiry Ntuh AthryNo ratings yet
- Art Appreciation Chapter 3 SummaryDocument6 pagesArt Appreciation Chapter 3 SummaryDiego A. Odchimar IIINo ratings yet
- Reference GuideDocument88 pagesReference GuideAnonymous Qm0zbNk100% (1)
- Vanguard 44 - Anti Tank Helicopters PDFDocument48 pagesVanguard 44 - Anti Tank Helicopters PDFsoljenitsin250% (2)
- Kootenay Lake Pennywise April 26, 2016Document48 pagesKootenay Lake Pennywise April 26, 2016Pennywise PublishingNo ratings yet