You might also like
- 2018 ESC-EACTS Guidelines On Myocardial RevascularizationDocument96 pages2018 ESC-EACTS Guidelines On Myocardial RevascularizationTony Miguel Saba SabaNo ratings yet
- Hipogonadismo MasculinoDocument2 pagesHipogonadismo MasculinoTony Miguel Saba SabaNo ratings yet
- Prioritising Risk Factors For Type 2 Diabetes Causal Inference Through Genetic ApproachesDocument10 pagesPrioritising Risk Factors For Type 2 Diabetes Causal Inference Through Genetic ApproachesTony Miguel Saba SabaNo ratings yet
- Effects of Weight Loss On Acoustic Parameters After Bariatric SurgeryDocument2 pagesEffects of Weight Loss On Acoustic Parameters After Bariatric SurgeryTony Miguel Saba SabaNo ratings yet
- Disminucion de Lípidos en Sindrome Coronario Agudo. Nicholls S 2018Document2 pagesDisminucion de Lípidos en Sindrome Coronario Agudo. Nicholls S 2018Tony Miguel Saba SabaNo ratings yet
- Conversion From Insulin Glargine U-100 To Insulin Glargine U-300 or Insulin Degludec and The Impact On Dosage RequirementsDocument9 pagesConversion From Insulin Glargine U-100 To Insulin Glargine U-300 or Insulin Degludec and The Impact On Dosage RequirementsTony Miguel Saba SabaNo ratings yet
- Predictors of Success in Bariatric Surgery The Role of BMI and Pre-Operative ComorbiditiesDocument7 pagesPredictors of Success in Bariatric Surgery The Role of BMI and Pre-Operative ComorbiditiesTony Miguel Saba SabaNo ratings yet
- Bariatric Surgery As An Efficient Treatment For Non-Alcoholic Fatty Liver Disease in A Prospective Study With 1-Year Follow-UpDocument9 pagesBariatric Surgery As An Efficient Treatment For Non-Alcoholic Fatty Liver Disease in A Prospective Study With 1-Year Follow-UpTony Miguel Saba SabaNo ratings yet
- Literatura en La Web Asociada A Cirugía BariátricaDocument8 pagesLiteratura en La Web Asociada A Cirugía BariátricaTony Miguel Saba SabaNo ratings yet
- Effects of Weight Loss On Acoustic Parameters After Bariatric Surgery PDFDocument5 pagesEffects of Weight Loss On Acoustic Parameters After Bariatric Surgery PDFTony Miguel Saba SabaNo ratings yet
- Trueness Precision and Stability of The LIAISON 1-84 Parathyroid Hormone (PTH) Third-GeneratDocument7 pagesTrueness Precision and Stability of The LIAISON 1-84 Parathyroid Hormone (PTH) Third-GeneratTony Miguel Saba SabaNo ratings yet
- Elipse Balloon The Pitfalls of Excessive SimplicityDocument3 pagesElipse Balloon The Pitfalls of Excessive SimplicityTony Miguel Saba SabaNo ratings yet
- The Curious Case of Postprandial Glucose Less Than Fasting Glucose Little Things That Matter MuchDocument3 pagesThe Curious Case of Postprandial Glucose Less Than Fasting Glucose Little Things That Matter MuchTony Miguel Saba SabaNo ratings yet
- Pituitary Tumour Apoplexy Within Prolactinomas in Children A More Aggressive ConditionDocument6 pagesPituitary Tumour Apoplexy Within Prolactinomas in Children A More Aggressive ConditionTony Miguel Saba SabaNo ratings yet
- Diagnosis and Management of Neuropathic ItchDocument12 pagesDiagnosis and Management of Neuropathic ItchTony Miguel Saba SabaNo ratings yet
- Drugs On The Horizon For Chronic PruritusDocument10 pagesDrugs On The Horizon For Chronic PruritusTony Miguel Saba SabaNo ratings yet
- Glucagon Prescriptions For Diabetes Patients After Emergency Department Visits For HypoglycemiaDocument17 pagesGlucagon Prescriptions For Diabetes Patients After Emergency Department Visits For HypoglycemiaTony Miguel Saba SabaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Pediatrics in Review 2012 McCavit 195 206Document14 pagesPediatrics in Review 2012 McCavit 195 206cindyNo ratings yet
- Movement Disorders Types - Mayo ClinicDocument1 pageMovement Disorders Types - Mayo ClinicdrrajmptnNo ratings yet
- Cat BreedsDocument13 pagesCat Breedsprabhakar_n1No ratings yet
- Case Presentation CA MammaeDocument17 pagesCase Presentation CA Mammaefrili adriaNo ratings yet
- GenpathDocument10 pagesGenpathNatural Science BiologyNo ratings yet
- Microbial Growth PhaseDocument2 pagesMicrobial Growth PhaseMahathir Mohmed100% (5)
- 20.2 Biotechnology - and - Genetic - Engineering - Igcse Cie Biology - Ext Theory QPDocument9 pages20.2 Biotechnology - and - Genetic - Engineering - Igcse Cie Biology - Ext Theory QPBlessing TshumaNo ratings yet
- Current Status and Prospective of Cancer Disease in Bangladesh: A Cross-Sectional SurveyDocument7 pagesCurrent Status and Prospective of Cancer Disease in Bangladesh: A Cross-Sectional SurveyIOSR Journal of Pharmacy100% (1)
- Topic 5 MsDocument22 pagesTopic 5 Msbody fayezNo ratings yet
- Đề Thi Hsg Tiếng Anh Vĩnh Phúc (Lớp 12)Document8 pagesĐề Thi Hsg Tiếng Anh Vĩnh Phúc (Lớp 12)Cù Minh HiếuNo ratings yet
- The Dog Encyclopedia (VetBooks - Ir)Document362 pagesThe Dog Encyclopedia (VetBooks - Ir)miki122295% (22)
- Electrical Activity of The HeartDocument47 pagesElectrical Activity of The HeartSodeinde SimeonNo ratings yet
- Free Microbiology Practice Questions - Help Your Microbiology Test ScoreDocument3 pagesFree Microbiology Practice Questions - Help Your Microbiology Test ScoreDalbir SinghNo ratings yet
- Roche GlucoseDocument4 pagesRoche GlucoseDiep LeNo ratings yet
- Lens Related GlaucomaDocument19 pagesLens Related GlaucomaUsama ButtNo ratings yet
- QuinonesDocument2 pagesQuinonessuresh100% (1)
- Bin Wu - New Discoveries in Embryology (2015, InTech)Document261 pagesBin Wu - New Discoveries in Embryology (2015, InTech)Katy A100% (1)
- 2.5.9 Genetic EngineeringDocument6 pages2.5.9 Genetic EngineeringGeorge Oswald Junior CarringtonNo ratings yet
- Anatomy and Biomechanics of The Meniscus, Allen, OTO95+Document8 pagesAnatomy and Biomechanics of The Meniscus, Allen, OTO95+Ana María RodríguezNo ratings yet
- Cerebral Plasticity: Windows of Opportunity in The Developing BrainDocument26 pagesCerebral Plasticity: Windows of Opportunity in The Developing BrainRebeca FloresNo ratings yet
- Autism AmishDocument2 pagesAutism AmishPower one100% (1)
- Stenotrophomona Maltophilia y Bulkorelia Cepacia. Mnadell 2009Document8 pagesStenotrophomona Maltophilia y Bulkorelia Cepacia. Mnadell 2009Laura López Del Castillo LalydelcaNo ratings yet
- Unit 4 Notes Edexcel BiologyDocument19 pagesUnit 4 Notes Edexcel BiologyAe Banpong69% (13)
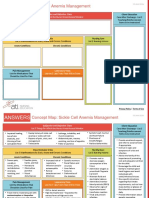
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 pagesNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- Prevalence and Species Spectrum of Pulmonary Nontuberculous Mycobacteria Isolates at A Tertiary Care CenterDocument6 pagesPrevalence and Species Spectrum of Pulmonary Nontuberculous Mycobacteria Isolates at A Tertiary Care CenterHiroj BagdeNo ratings yet
- Online ENVR 1401-Natural Selection Lab-Text Only-JcDocument9 pagesOnline ENVR 1401-Natural Selection Lab-Text Only-Jcsameer100% (1)
- Cell Power ManualDocument95 pagesCell Power ManualKeith McFarlaneNo ratings yet
- Topik 8 Recombinant Dna Technologies Soalan ObjectiveDocument5 pagesTopik 8 Recombinant Dna Technologies Soalan ObjectiveIslah100% (1)
- Aphasia and DyslexiaDocument17 pagesAphasia and DyslexiaMary Christine GonzalesNo ratings yet
- Forensic Notes PDFDocument155 pagesForensic Notes PDFSoni Mahendran100% (1)