You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Ultimate Guide To Starting Your First Ecommerce Business PDFDocument86 pagesThe Ultimate Guide To Starting Your First Ecommerce Business PDFzim1992No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Gait Analysis PresentationDocument41 pagesGait Analysis PresentationKýñg ButlerNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Expert Advice On Choosing A Niche Our Top 32 e Commerce Niches Research and AnalysisDocument163 pagesExpert Advice On Choosing A Niche Our Top 32 e Commerce Niches Research and AnalysisDawud MuhammadNo ratings yet
- 702 Home Exercises Cardiac Rehabilitation Programme PDFDocument16 pages702 Home Exercises Cardiac Rehabilitation Programme PDFSMI 93No ratings yet
- Shoe GuideDocument9 pagesShoe Guidemohamed rabie AllaouaNo ratings yet
- Fundamentals of Insight Meditation - Mahasi Sayadaw-1959Document56 pagesFundamentals of Insight Meditation - Mahasi Sayadaw-1959BuddhaDhammaSangahNo ratings yet
- Human Walking RoseDocument248 pagesHuman Walking RosePablo CruzNo ratings yet
- Physical Therapy Protocol For Acute Care Adult HemiplegiaDocument12 pagesPhysical Therapy Protocol For Acute Care Adult Hemiplegiaj_______________jNo ratings yet
- WalkerDocument18 pagesWalkerNini JendeukieNo ratings yet
- 1102 Neurons and NeurotransmittersDocument28 pages1102 Neurons and NeurotransmittersDawud MuhammadNo ratings yet
- The Application of Islamic Legal Maxims To Islamic Banking and FinanceDocument22 pagesThe Application of Islamic Legal Maxims To Islamic Banking and FinanceNuraddin Abdi Elmi93% (15)
- Harris Hip ScoreDocument2 pagesHarris Hip ScoreEma Abrudan100% (1)
- Top 5 Ecommerce PlatformsDocument16 pagesTop 5 Ecommerce PlatformsDawud Muhammad100% (1)
- Ethica CIFE Study NotesDocument85 pagesEthica CIFE Study NotesSolomon TekalignNo ratings yet
- Degreeworks Graduation Plan 3 Year Plan Name: Spring 2018Document5 pagesDegreeworks Graduation Plan 3 Year Plan Name: Spring 2018Dawud MuhammadNo ratings yet
- Excel LAbDocument5 pagesExcel LAbDawud MuhammadNo ratings yet
- Put Your Drone To Work PDFDocument10 pagesPut Your Drone To Work PDFDawud Muhammad100% (1)
- Demystifying Islamic FinanceDocument44 pagesDemystifying Islamic FinancesafdarnobodyNo ratings yet
- 08 - Strategic Trends in The Islamic Banking and Finance MovementDocument9 pages08 - Strategic Trends in The Islamic Banking and Finance MovementDawud MuhammadNo ratings yet
- A Simple Figh and Economics Rationale For Mutualization in Islamic Financial Inter MediationDocument10 pagesA Simple Figh and Economics Rationale For Mutualization in Islamic Financial Inter MediationHeidi FreeNo ratings yet
- 03 - A Basic Guide To Contemporary Islamic Banking and FinanceDocument18 pages03 - A Basic Guide To Contemporary Islamic Banking and FinanceDawud MuhammadNo ratings yet
- The Effect of Gait Training and Exercise Programs On Gait and Balance in Post-Stroke PatientsDocument5 pagesThe Effect of Gait Training and Exercise Programs On Gait and Balance in Post-Stroke PatientsDawud MuhammadNo ratings yet
- 07 Shari'Ah Islamic BankingDocument14 pages07 Shari'Ah Islamic BankingDawud MuhammadNo ratings yet
- Islamic Banking DefinitionsDocument7 pagesIslamic Banking Definitionsjuni26287No ratings yet
- Abozaid, Abduzlazeem - PresentationDocument11 pagesAbozaid, Abduzlazeem - PresentationjavedkaleemNo ratings yet
- 07 Shari'Ah Islamic BankingDocument14 pages07 Shari'Ah Islamic BankingDawud MuhammadNo ratings yet
- 05 - Shari'ah and Legal Issues of Online Islamic Banking and FinanceDocument10 pages05 - Shari'ah and Legal Issues of Online Islamic Banking and FinanceDawud MuhammadNo ratings yet
- Course SyllabusDocument24 pagesCourse SyllabusDawud MuhammadNo ratings yet
- Islamic Banking PrimerDocument49 pagesIslamic Banking Primerchughtai2000No ratings yet
- ITEC1001 Fall 2018 ScheduleDocument31 pagesITEC1001 Fall 2018 ScheduleDawud MuhammadNo ratings yet
- Parts of The BrainDocument32 pagesParts of The BrainDawud MuhammadNo ratings yet
- The Effect of Gait Training and Exercise - Post-StrokeDocument23 pagesThe Effect of Gait Training and Exercise - Post-StrokeDawud MuhammadNo ratings yet
- GAITDocument1 pageGAITDawud MuhammadNo ratings yet
- American Posture Institute GuideDocument17 pagesAmerican Posture Institute GuidesololuiNo ratings yet
- 100 Things To Sell in 2017Document9 pages100 Things To Sell in 2017MuhammadZaydArattKhanNo ratings yet
- Exercises For Lower-Limb Amputees: Gait TrainingDocument76 pagesExercises For Lower-Limb Amputees: Gait TrainingInternational Committee of the Red Cross100% (1)
- The Effect of Gait Training and Exercise Programs On Gait and Balance in Post-Stroke PatientsDocument5 pagesThe Effect of Gait Training and Exercise Programs On Gait and Balance in Post-Stroke PatientsDawud MuhammadNo ratings yet
- American Posture Institute GuideDocument17 pagesAmerican Posture Institute GuidesololuiNo ratings yet
- Kaye Walker: Swivel Front Wheels Can Be Locked in A Fixed PositionDocument13 pagesKaye Walker: Swivel Front Wheels Can Be Locked in A Fixed PositionMir Habib KurdNo ratings yet
- Pertemuan 9 Arista PDFDocument12 pagesPertemuan 9 Arista PDFNi Putu aristaNo ratings yet
- Physical Activity - MotivationDocument2 pagesPhysical Activity - Motivationapi-471785672No ratings yet
- Simulating The First Steps of A Walking Hexapod RobotDocument71 pagesSimulating The First Steps of A Walking Hexapod Robotbahamut518No ratings yet
- Cathelyn TimpleDocument26 pagesCathelyn TimpleCarlos Arturo Franco del MoralNo ratings yet
- Air Jordan - 4Document4 pagesAir Jordan - 4Saldi RNo ratings yet
- An Approach To Drastically Reduce The Required Legs Dofs For Bipedal Robots and Lower Limb ExoskeletonsDocument15 pagesAn Approach To Drastically Reduce The Required Legs Dofs For Bipedal Robots and Lower Limb ExoskeletonsRenatoNo ratings yet
- Caso Alden RealizarDocument30 pagesCaso Alden RealizarMarlon Yesid Buitrago SanchezNo ratings yet
- SOT Wedding Shoes Price List Update September2022Document6 pagesSOT Wedding Shoes Price List Update September2022maria yasintaNo ratings yet
- Mitochondrial Myopathy: How Exercise Can HelpDocument36 pagesMitochondrial Myopathy: How Exercise Can HelpSri HariNo ratings yet
- HPE 660 Lecture 6 - Intro To GaitDocument20 pagesHPE 660 Lecture 6 - Intro To GaitTrevor SmedaNo ratings yet
- Id Company Name Address PincodeDocument4 pagesId Company Name Address PincodeAmresh AgrahariNo ratings yet
- Transportation Research Part B: Ren-Yong Guo, Hai-Jun Huang, S.C. WongDocument17 pagesTransportation Research Part B: Ren-Yong Guo, Hai-Jun Huang, S.C. WongKhairulNo ratings yet
- UPS RulesDocument5 pagesUPS RulesJovon StigerNo ratings yet
- Walking Festival Booklet 2016 WEBDocument15 pagesWalking Festival Booklet 2016 WEBmiller999No ratings yet
- Post Operative Management - TKRDocument31 pagesPost Operative Management - TKRselva5252No ratings yet
- Case Study: WhatDocument3 pagesCase Study: WhatAbdul Razzaq AfridiNo ratings yet
- Injury-Free Small FileDocument65 pagesInjury-Free Small FileGeorge PNFNo ratings yet
- ROADMAP Report A2 Worksheet UnitDocument2 pagesROADMAP Report A2 Worksheet UnitWayra SonqoyNo ratings yet
- Research Paper On Klann MechanismDocument8 pagesResearch Paper On Klann Mechanismaflbtcxfc100% (1)
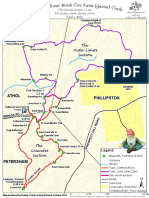
- The Cutthroat Brook Tree Farm (Gnome) TrailsDocument2 pagesThe Cutthroat Brook Tree Farm (Gnome) TrailsZachary DeLucaNo ratings yet
- Gait & Posture Volume Issue 2018 - Gluteal Tendinopathy and Hip Osteoarthritis - Different PatholDocument23 pagesGait & Posture Volume Issue 2018 - Gluteal Tendinopathy and Hip Osteoarthritis - Different PatholGiancarlo Gardella MartínezNo ratings yet