You might also like
- Clozapine: SchizophrenicDocument8 pagesClozapine: SchizophrenicVictoria FellowsNo ratings yet
- Kane1988 PDFDocument8 pagesKane1988 PDFRavi KumarNo ratings yet
- Clozapine and Haloperidol in ModeratelyDocument8 pagesClozapine and Haloperidol in Moderatelyrinaldiapt08No ratings yet
- Stroup2019 PDFDocument2 pagesStroup2019 PDFGrayfox89No ratings yet
- 23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25Document5 pages23 Ifteni Tit Rápida 1 Acta - Psychiatrica - Scandinavica - 2014 - 130 - (1) - 25observacionfray23No ratings yet
- Clozapina 2Document12 pagesClozapina 2Robert MovileanuNo ratings yet
- The Effects of Clozapine On Alcohol and Drug Use Disorders Among Patients With SchizophreniaDocument10 pagesThe Effects of Clozapine On Alcohol and Drug Use Disorders Among Patients With SchizophreniaEcaNo ratings yet
- Management of Clozapine-Resistant Schizophrenia: Rob W. Kerwin & Anusha BolonnaDocument6 pagesManagement of Clozapine-Resistant Schizophrenia: Rob W. Kerwin & Anusha Bolonnaatika ichaNo ratings yet
- Clozapine Use in A CohortDocument6 pagesClozapine Use in A CohortcaturNo ratings yet
- Comparative Effectiveness of Clozapine and Standard Antipsychotic Treatment in Adults With SchizophreniaDocument8 pagesComparative Effectiveness of Clozapine and Standard Antipsychotic Treatment in Adults With SchizophreniaOkky AlfianNo ratings yet
- Nejm 199709183371202Document7 pagesNejm 199709183371202Nurul UlfaNo ratings yet
- Clozapin RisperidonDocument7 pagesClozapin RisperidonAnonymous 2LcGdsRNo ratings yet
- Clozapine Augementation in CRSDocument12 pagesClozapine Augementation in CRSMarius PaţaNo ratings yet
- Clozapina Si RisperidonaDocument17 pagesClozapina Si RisperidonaRobert MovileanuNo ratings yet
- Recommendations For Antipsychotic Selection in Schizophrenia and Schizoaffective Disorders June 2012Document5 pagesRecommendations For Antipsychotic Selection in Schizophrenia and Schizoaffective Disorders June 2012Kunthi Kencana Makayasa PutriNo ratings yet
- Knowledge Notes - Catie and Cutlass SummaryDocument3 pagesKnowledge Notes - Catie and Cutlass SummaryvinodksahuNo ratings yet
- ClozapineDocument5 pagesClozapineANDREWNo ratings yet
- A Retrospective Cohort Study of Diabetes Mellitus and Antipsychotic Treatment in The United StatesDocument7 pagesA Retrospective Cohort Study of Diabetes Mellitus and Antipsychotic Treatment in The United StatesDeegh MudhaNo ratings yet
- Cuma Abstraknya Aja: TTG Risperidone: Stroke Therapy TreatmentsDocument6 pagesCuma Abstraknya Aja: TTG Risperidone: Stroke Therapy TreatmentsChandz ChanDra ErryandariNo ratings yet
- Clozapine in Treatment of Schizophrenia: V. Burtea P. Ifteni A Teodorescu L. RogozeaDocument6 pagesClozapine in Treatment of Schizophrenia: V. Burtea P. Ifteni A Teodorescu L. RogozeaReza Badruun Syahrul HakimNo ratings yet
- Second and Third Generation Antipsychotics: A Comprehensive HandbookFrom EverandSecond and Third Generation Antipsychotics: A Comprehensive HandbookRating: 5 out of 5 stars5/5 (1)
- Jurnal SkizoafektifDocument7 pagesJurnal SkizoafektifkhairinanurulNo ratings yet
- The Choice of Drugs For Schizophrenia: New England Journal MedicineDocument3 pagesThe Choice of Drugs For Schizophrenia: New England Journal Medicinewiwin09No ratings yet
- Evaluation of Treatment-Resistant SchizophreniaDocument12 pagesEvaluation of Treatment-Resistant SchizophreniaFlo RenceNo ratings yet
- JURNAL ASLI FarmakoterapiDocument4 pagesJURNAL ASLI FarmakoterapiWulandiraNo ratings yet
- Atypical Antipsychotic Augmentation in Major Depressive DisorderDocument13 pagesAtypical Antipsychotic Augmentation in Major Depressive DisorderrantiNo ratings yet
- TreatmentResistantSchizophreniaReview CITROME Neuropsych2011Document23 pagesTreatmentResistantSchizophreniaReview CITROME Neuropsych2011Leslie CitromeNo ratings yet
- Clozapine v. First and Second Generation Antipsychotics in Treatment-Refractory Schizophrenia Systematic Review and Meta-AnalysisDocument18 pagesClozapine v. First and Second Generation Antipsychotics in Treatment-Refractory Schizophrenia Systematic Review and Meta-AnalysisElianAmadeaNo ratings yet
- Schizophrenia Treatment & Management - Approach Considerations, Antipsychotic Pharmacotherapy, Other PharmacotherapyDocument13 pagesSchizophrenia Treatment & Management - Approach Considerations, Antipsychotic Pharmacotherapy, Other PharmacotherapydilaNo ratings yet
- Antipsychotic Medication in Schizophrenia - A ReviewDocument11 pagesAntipsychotic Medication in Schizophrenia - A Reviewrisang akrima fikriNo ratings yet
- A Rational Use of Clozapine Based On Adverse Drug Reactions, Pharmacokinetics, and Clinical PharmacopsychologyDocument15 pagesA Rational Use of Clozapine Based On Adverse Drug Reactions, Pharmacokinetics, and Clinical PharmacopsychologyDian GbligNo ratings yet
- 1286 The Choice of Anti Psychotic Drugs For SchizopheniaDocument3 pages1286 The Choice of Anti Psychotic Drugs For SchizopheniaYbeth Luna SolisNo ratings yet
- Jurnal 4Document12 pagesJurnal 4Muhammad Andika PerdanaNo ratings yet
- The Choice of Antipsychotic Drugs For Schizophrenia: EditorialsDocument3 pagesThe Choice of Antipsychotic Drugs For Schizophrenia: EditorialsIlham WahyuNo ratings yet
- Clozapine Augmented With Risperidone in The Treatment of Schizophrenia: A Randomized, Double-Blind, Placebo-Controlled TrialDocument8 pagesClozapine Augmented With Risperidone in The Treatment of Schizophrenia: A Randomized, Double-Blind, Placebo-Controlled TrialIga Faldini GazaliNo ratings yet
- The Treatment of SchizophreniaDocument9 pagesThe Treatment of Schizophreniaapi-542787928No ratings yet
- Comparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaDocument6 pagesComparison Between Clozapine, An Atypical Antipsychotic Agent and Haloperidol, A Conventional Agent Used To Treat SchizophreniaLonkesNo ratings yet
- Lally 2015Document11 pagesLally 2015Mariana PestanaNo ratings yet
- Alternative Medicine - Medical Marijuana News - Cannabinoids On Trial For Multiple SclerosisDocument1 pageAlternative Medicine - Medical Marijuana News - Cannabinoids On Trial For Multiple Sclerosisfreed1No ratings yet
- Multiple Versus Single Antipsychotic Agents For Hospitalized Psychiatric Patients: Case-Control Study of Risks Versus BenefitsDocument7 pagesMultiple Versus Single Antipsychotic Agents For Hospitalized Psychiatric Patients: Case-Control Study of Risks Versus BenefitsPutri KeyshaNo ratings yet
- Smelson Et Al 2002 Risperidone Decreases Craving and Relapses in Individuals With Schizophrenia and Cocaine DependenceDocument5 pagesSmelson Et Al 2002 Risperidone Decreases Craving and Relapses in Individuals With Schizophrenia and Cocaine Dependence20WH1A0557 KASHETTY DEEKSHITHANo ratings yet
- Relationship of Atypical Antipsychotics With Development of Diabetes MellitusDocument9 pagesRelationship of Atypical Antipsychotics With Development of Diabetes MellitusLeslie CitromeNo ratings yet
- Use of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaDocument4 pagesUse of Very-High-Dose Olanzapine in Treatment-Resistant SchizophreniaPutu Agus GrantikaNo ratings yet
- Treatments For Schizophrenia: A Critical Review of Pharmacology and Mechanisms of Action of Antipsychotic DrugsDocument26 pagesTreatments For Schizophrenia: A Critical Review of Pharmacology and Mechanisms of Action of Antipsychotic DrugsMaria Jose CastañedaNo ratings yet
- Antipsychotic Augmentation vs. Monotherapy in Schizophrenia: Systematic Review, Meta-Analysis and Meta-Regression AnalysisDocument13 pagesAntipsychotic Augmentation vs. Monotherapy in Schizophrenia: Systematic Review, Meta-Analysis and Meta-Regression AnalysisvanfafiafiaNo ratings yet
- Antipsychotic Augmentation vs. Monotherapy in Schizophrenia: Systematic Review, Meta-Analysis and Meta-Regression AnalysisDocument13 pagesAntipsychotic Augmentation vs. Monotherapy in Schizophrenia: Systematic Review, Meta-Analysis and Meta-Regression AnalysisvanfafiafiaNo ratings yet
- Herrmann WM, Stephan K. Int Psychogeriatr. 1992 4 (1) :25-44.Document20 pagesHerrmann WM, Stephan K. Int Psychogeriatr. 1992 4 (1) :25-44.Ангелина СкоморохинаNo ratings yet
- CAFE Study Full ProtocolDocument51 pagesCAFE Study Full ProtocolMarkingsonCase100% (1)
- Multiple Versus Single Antipsychotic Agents For Hospitalized Psychiatric Patients: Case-Control Study of Risks Versus BenefitsDocument7 pagesMultiple Versus Single Antipsychotic Agents For Hospitalized Psychiatric Patients: Case-Control Study of Risks Versus BenefitsPutri KeyshaNo ratings yet
- Pone 0003150 PDFDocument5 pagesPone 0003150 PDFAnonymous hvOuCjNo ratings yet
- Kontaxakis 2006Document6 pagesKontaxakis 2006citra kurnia pratiwiNo ratings yet
- Journal ClubDocument63 pagesJournal Clubdrkadiyala2No ratings yet
- P 007 OlanzapineDocument11 pagesP 007 OlanzapineBalasubrahmanya K. R.No ratings yet
- CATIE Trial Summary PaperDocument14 pagesCATIE Trial Summary PaperNim RodNo ratings yet
- Epi Drugs EficaciesDocument18 pagesEpi Drugs EficaciesaandreiiNo ratings yet
- Focus On The Clinical Ramifications of Antipsychotic Choice For The Risk For Developing Type 2 Diabetes MellitusDocument5 pagesFocus On The Clinical Ramifications of Antipsychotic Choice For The Risk For Developing Type 2 Diabetes MellitusLeslie CitromeNo ratings yet
- Lobos JA Et Al 2010Document191 pagesLobos JA Et Al 2010Evi LoNo ratings yet
- Clotiapine - Another Forgotten Treassure in PsychiatryDocument1 pageClotiapine - Another Forgotten Treassure in PsychiatryJuan IgnacioNo ratings yet
- Effect OF Chlorpromazine AND Haloperidol Combination ON Lipid Profile IN Nigeria Schizophrenic PatientsDocument10 pagesEffect OF Chlorpromazine AND Haloperidol Combination ON Lipid Profile IN Nigeria Schizophrenic PatientstrianaamaliaNo ratings yet
- Treatment–Refractory Schizophrenia: A Clinical ConundrumFrom EverandTreatment–Refractory Schizophrenia: A Clinical ConundrumPeter F. BuckleyNo ratings yet
- Central Venous Access Device (CVAD) ManagementDocument77 pagesCentral Venous Access Device (CVAD) ManagementEvaG2012No ratings yet
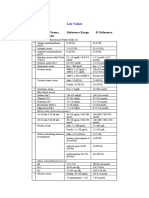
- Blood, Plasma, Serum Reference Range SI Reference: Lab ValuesDocument4 pagesBlood, Plasma, Serum Reference Range SI Reference: Lab ValuesEvaG2012No ratings yet
- SyphilisDocument24 pagesSyphilisEvaG2012No ratings yet
- Between The Flags PDFDocument2 pagesBetween The Flags PDFEvaG2012No ratings yet
- Radiology Five Basic Radiographic DensitiesDocument1 pageRadiology Five Basic Radiographic DensitiesEvaG2012No ratings yet
- Techniques For Analysing Visual TextsDocument4 pagesTechniques For Analysing Visual TextsEvaG2012No ratings yet
- NURS FPX 6021 Assessment 1 Concept MapDocument7 pagesNURS FPX 6021 Assessment 1 Concept MapCarolyn HarkerNo ratings yet
- Sycip v. CA (Sufficient Funds With The Drawee Bank)Document15 pagesSycip v. CA (Sufficient Funds With The Drawee Bank)Arnold BagalanteNo ratings yet
- Manual StereoDocument29 pagesManual StereoPeter Mac RedNo ratings yet
- Economic Survey 2023 2Document510 pagesEconomic Survey 2023 2esr47No ratings yet
- Jesus Hold My Hand EbDocument2 pagesJesus Hold My Hand EbGregg100% (3)
- Army War College PDFDocument282 pagesArmy War College PDFWill100% (1)
- Filipino Chicken Cordon BleuDocument7 pagesFilipino Chicken Cordon BleuHazel Castro Valentin-VillamorNo ratings yet
- Sugar Industries of PakistanDocument19 pagesSugar Industries of Pakistanhelperforeu50% (2)
- Horgolás Minta - PulcsiDocument5 pagesHorgolás Minta - PulcsiCagey Ice-RoyNo ratings yet
- Especificação - PneusDocument10 pagesEspecificação - Pneusmarcos eduNo ratings yet
- Agrarian ReformDocument40 pagesAgrarian ReformYannel Villaber100% (2)
- PH Water On Stability PesticidesDocument6 pagesPH Water On Stability PesticidesMontoya AlidNo ratings yet
- January Payslip 2023.pdf - 1-2Document1 pageJanuary Payslip 2023.pdf - 1-2Arbaz KhanNo ratings yet
- Deep MethodDocument13 pagesDeep Methoddarkelfist7No ratings yet
- OrderFlow Charts and Notes 19th Sept 17 - VtrenderDocument9 pagesOrderFlow Charts and Notes 19th Sept 17 - VtrenderSinghRaviNo ratings yet
- A Comparison of Practitioner and Student WritingDocument28 pagesA Comparison of Practitioner and Student WritingMichael Sniper WuNo ratings yet
- 1 Intro To Society, Community and EducationDocument29 pages1 Intro To Society, Community and EducationMaria Michelle A. Helar100% (1)
- ReproTech, LLC Welcomes New President & CEO, William BraunDocument3 pagesReproTech, LLC Welcomes New President & CEO, William BraunPR.comNo ratings yet
- The Problem Between Teacher and Students: Name: Dinda Chintya Sinaga (2152121008) Astry Iswara Kelana Citra (2152121005)Document3 pagesThe Problem Between Teacher and Students: Name: Dinda Chintya Sinaga (2152121008) Astry Iswara Kelana Citra (2152121005)Astry Iswara Kelana CitraNo ratings yet
- E F Eng l1 l2 Si 011Document2 pagesE F Eng l1 l2 Si 011Simona ButeNo ratings yet
- ANTH 222 Syllabus 2012Document6 pagesANTH 222 Syllabus 2012Maythe S. HanNo ratings yet
- Bus Organization of 8085 MicroprocessorDocument6 pagesBus Organization of 8085 MicroprocessorsrikrishnathotaNo ratings yet
- Law - Midterm ExamDocument2 pagesLaw - Midterm ExamJulian Mernando vlogsNo ratings yet
- HP MSM775 ZL Controller Installation GuideDocument21 pagesHP MSM775 ZL Controller Installation GuidezarandijaNo ratings yet
- Review of Related LiteratureDocument9 pagesReview of Related LiteratureMarion Joy GanayoNo ratings yet
- Test Bank For Cognitive Psychology Connecting Mind Research and Everyday Experience 3rd Edition e Bruce GoldsteinDocument24 pagesTest Bank For Cognitive Psychology Connecting Mind Research and Everyday Experience 3rd Edition e Bruce GoldsteinMichaelThomasyqdi100% (49)
- Highway Capacity ManualDocument13 pagesHighway Capacity Manualgabriel eduardo carmona joly estudianteNo ratings yet
- Hayat ProposalDocument22 pagesHayat Proposalsebehadinahmed1992No ratings yet
- FFT SlidesDocument11 pagesFFT Slidessafu_117No ratings yet
- Kindergarten Report Card SampleDocument3 pagesKindergarten Report Card Sampleapi-294165063No ratings yet