You might also like
- Overview Antenatal CareDocument54 pagesOverview Antenatal CareRizky Dwidya AmirtasariNo ratings yet
- AUB StartedDocument13 pagesAUB StartedIbrahim AbdullahNo ratings yet
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- Urinary Tract Infections Pregnancy PDFDocument19 pagesUrinary Tract Infections Pregnancy PDFNay Lin HtikeNo ratings yet
- Myop in PregnancyDocument4 pagesMyop in PregnancySamuel WilliamsNo ratings yet
- Fetal Physiological Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological MeasurementsFrom EverandFetal Physiological Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological MeasurementsPeter RolfeNo ratings yet
- Judi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009Document66 pagesJudi Januadi Endjun: Gatot Soebroto Army Central Hospital/ Medical Faculty, University of Indonesia ISUOG, Bali, 2009emilyakmanNo ratings yet
- Infertility IDocument36 pagesInfertility Idr_asaleh100% (1)
- Fetal Growth Restriction ACOG 2013Document12 pagesFetal Growth Restriction ACOG 2013Maverick 18100% (3)
- Green Top Guidelines 13Document29 pagesGreen Top Guidelines 13garfield1No ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2No ratings yet
- 2019 PreeclampsiaDocument19 pages2019 PreeclampsiaMalexandra S CandoNo ratings yet
- Obs History Taking FormatDocument24 pagesObs History Taking FormatBibek PandeyNo ratings yet
- Practice Bulletin: Antiphospholipid SyndromeDocument8 pagesPractice Bulletin: Antiphospholipid SyndromeSus ArNo ratings yet
- Preterm Labour: Management GuidelinesDocument44 pagesPreterm Labour: Management Guidelinesvacha sardarNo ratings yet
- Acute Abdomen During Pregnancy BelaynehDocument47 pagesAcute Abdomen During Pregnancy BelaynehYohannis AsefaNo ratings yet
- Rcog PpromDocument7 pagesRcog PpromDevi SyamNo ratings yet
- Twin PregnancyDocument73 pagesTwin Pregnancykrishna mandalNo ratings yet
- Acog Vbac PDFDocument14 pagesAcog Vbac PDFFrancyn Rossi YangsonNo ratings yet
- SOGC Guideline for Managing Uterine FibroidsDocument22 pagesSOGC Guideline for Managing Uterine FibroidsSarah MuharomahNo ratings yet
- MRCOG Part 1 Exam Module SummaryDocument4 pagesMRCOG Part 1 Exam Module SummaryAmadeus KQNo ratings yet
- Cardiac Disease and Pregnancy RCOG GuidelineDocument18 pagesCardiac Disease and Pregnancy RCOG GuidelinedanielsusenoNo ratings yet
- Jurnal Inggris PDFDocument4 pagesJurnal Inggris PDFTom PrasNo ratings yet
- Threatened AbortionDocument1 pageThreatened AbortionKEn PilapilNo ratings yet
- Dewhurst's Textbook of Obstetrics & GynaecologyFrom EverandDewhurst's Textbook of Obstetrics & GynaecologyChristoph LeesRating: 2 out of 5 stars2/5 (1)
- Deep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateDocument11 pagesDeep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateGabyta007No ratings yet
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- Antiphospholipid Syndrome in Pregnancy: Review of Diagnosis and TreatmentDocument7 pagesAntiphospholipid Syndrome in Pregnancy: Review of Diagnosis and TreatmentDara Dasawulansari SyamsuriNo ratings yet
- Impey Obs and Gynae Revision Notes PDFDocument9 pagesImpey Obs and Gynae Revision Notes PDFRoiseNo ratings yet
- Gestational Trophoblastic DiseasesDocument37 pagesGestational Trophoblastic DiseasesEdwin OkonNo ratings yet
- Abortion PresentationDocument46 pagesAbortion PresentationJhong Xyrus67% (3)
- Management of Borderline Ovarian Tumors - RCOGDocument6 pagesManagement of Borderline Ovarian Tumors - RCOGYossi Agung AriosenoNo ratings yet
- Fetal MonitoringDocument6 pagesFetal MonitoringRraouzmaaliNo ratings yet
- Obstetric Summm 1Document46 pagesObstetric Summm 1ملك عيسىNo ratings yet
- Singer and Monaghan's Cervical and Lower Genital Tract Precancer: Diagnosis and TreatmentFrom EverandSinger and Monaghan's Cervical and Lower Genital Tract Precancer: Diagnosis and TreatmentRating: 5 out of 5 stars5/5 (1)
- Handbook of Current and Novel Protocols for the Treatment of InfertilityFrom EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanNo ratings yet
- Recurrent MiscarriageDocument6 pagesRecurrent MiscarriageuzmajbnNo ratings yet
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocument27 pagesInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008No ratings yet
- Ovarian TorsionDocument48 pagesOvarian Torsionmaria ilyasNo ratings yet
- InfertilityDocument14 pagesInfertilityDrChauhanNo ratings yet
- Poly Hi DR AmnionDocument7 pagesPoly Hi DR Amnionwanwan_adongNo ratings yet
- Antepartum Fetal Surveillance ACOG Bulletin 2014 PDFDocument11 pagesAntepartum Fetal Surveillance ACOG Bulletin 2014 PDFDanNo ratings yet
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounNo ratings yet
- Tog Journal 2016Document61 pagesTog Journal 2016thevijay007100% (1)
- Reproductive Endocrinology FinalDocument98 pagesReproductive Endocrinology FinalChino Paolo SamsonNo ratings yet
- Fetal Monitoring Tests and TherapiesDocument46 pagesFetal Monitoring Tests and TherapiesAumrin Fathima100% (1)
- VBACDocument45 pagesVBACJuan Habli SoufalNo ratings yet
- Induction of Labor With Oxytocin - UpToDateDocument54 pagesInduction of Labor With Oxytocin - UpToDateJhoseline CamposNo ratings yet
- Cholestatic Disease in PregnancyDocument25 pagesCholestatic Disease in Pregnancyarifbotwin100% (1)
- Simposium 1 - Controversies - Dr. Teguh - HPV Vaccine Vs HPV Test-1Document20 pagesSimposium 1 - Controversies - Dr. Teguh - HPV Vaccine Vs HPV Test-1isnayu drNo ratings yet
- AUBDocument26 pagesAUByayaslaras96No ratings yet
- Hypertension in PregnancyDocument34 pagesHypertension in PregnancyMusekhirNo ratings yet
- Diabetes Acog 2017Document15 pagesDiabetes Acog 2017Holger Vicente Guerrero Guerrero100% (1)
- GLM0021 Postpartum Haemorrhage PDFDocument15 pagesGLM0021 Postpartum Haemorrhage PDFRubiahSheBiachNo ratings yet
- Referat: Abnormal Uerine Bleeding (AUB)Document28 pagesReferat: Abnormal Uerine Bleeding (AUB)Norbertus MacekaNo ratings yet
- Infertility: Reshmi SibyDocument80 pagesInfertility: Reshmi SibySusan ThomasNo ratings yet
- Multiple PregnancyDocument26 pagesMultiple PregnancyOmar mohamedNo ratings yet
- Genetics For MrcogDocument4 pagesGenetics For MrcogsriniNo ratings yet
- The Legal Perspective of Electronic Medical Records Implementation in TaiwanDocument67 pagesThe Legal Perspective of Electronic Medical Records Implementation in TaiwanEirna Syam Fitri IINo ratings yet
- 07-Vaccination Traveller RSUI 2020Document35 pages07-Vaccination Traveller RSUI 2020Eirna Syam Fitri IINo ratings yet
- Out 1 PDFDocument7 pagesOut 1 PDFEirna Syam Fitri IINo ratings yet
- Out 1 PDFDocument7 pagesOut 1 PDFEirna Syam Fitri IINo ratings yet
- Out 1 PDFDocument7 pagesOut 1 PDFEirna Syam Fitri IINo ratings yet
- PastedGraphic 1Document1 pagePastedGraphic 1Eirna Syam Fitri IINo ratings yet
- Tutorial Aik-Capital Budgeting DipakaiDocument11 pagesTutorial Aik-Capital Budgeting DipakaiEirna Syam Fitri IINo ratings yet
- Hasil PrepostestDocument1 pageHasil PrepostestEirna Syam Fitri IINo ratings yet
- EvakuasiDocument4 pagesEvakuasiRima DinaNo ratings yet
- Tutorial Aik-Capital Budgeting DipakaiDocument11 pagesTutorial Aik-Capital Budgeting DipakaiEirna Syam Fitri IINo ratings yet
- Prehospital Emergency Care Apr-Jun 2004 8, 2 Proquest Nursing & Allied Health SourceDocument4 pagesPrehospital Emergency Care Apr-Jun 2004 8, 2 Proquest Nursing & Allied Health SourceEirna Syam Fitri IINo ratings yet
- EvakuasiDocument4 pagesEvakuasiRima DinaNo ratings yet
- Water on the Brain Condition ExplainedDocument10 pagesWater on the Brain Condition ExplainedEirna Syam Fitri IINo ratings yet
- Water on the Brain Condition ExplainedDocument10 pagesWater on the Brain Condition ExplainedEirna Syam Fitri IINo ratings yet
- Record Blanks Print View - Life Sciences From Lafayette Instrument CompanyDocument2 pagesRecord Blanks Print View - Life Sciences From Lafayette Instrument CompanyEirna Syam Fitri IINo ratings yet
- Weight Gain Recommendations in PregnancyDocument4 pagesWeight Gain Recommendations in PregnancyEirna Syam Fitri IINo ratings yet
- HepatomegaliDocument6 pagesHepatomegaliEirna Syam Fitri IINo ratings yet
- Repairing Obstetric Anal Sphincter TearsDocument9 pagesRepairing Obstetric Anal Sphincter TearsEirna Syam Fitri IINo ratings yet
- RCT Platelet Transfusion in DengueDocument7 pagesRCT Platelet Transfusion in DengueEirna Syam Fitri IINo ratings yet
- Kortiko in DssDocument18 pagesKortiko in DssEirna Syam Fitri IINo ratings yet
- HepatomegaliDocument6 pagesHepatomegaliEirna Syam Fitri IINo ratings yet
- Dengue in PregnancyDocument4 pagesDengue in PregnancyEirna Syam Fitri IINo ratings yet
- Kortiko in DssDocument18 pagesKortiko in DssEirna Syam Fitri IINo ratings yet
- Vitamin DDocument7 pagesVitamin DEirna Syam Fitri IINo ratings yet
- Dengue in PregnancyDocument4 pagesDengue in PregnancyEirna Syam Fitri IINo ratings yet
- MULTIPLE INJURIES ASSOCIATED WITH SPINAL CORD TRAUMADocument11 pagesMULTIPLE INJURIES ASSOCIATED WITH SPINAL CORD TRAUMAEirna Syam Fitri IINo ratings yet
- Low Platelet Counts and Dengue Hemorrhagic FeverDocument6 pagesLow Platelet Counts and Dengue Hemorrhagic FeverEirna Syam Fitri IINo ratings yet
- Thrombocytopenia Associated With Dengue Hemorrhagic Fever Responds To Intravenous Administration of Anti-D (RH - D) Immune GlobulinDocument6 pagesThrombocytopenia Associated With Dengue Hemorrhagic Fever Responds To Intravenous Administration of Anti-D (RH - D) Immune GlobulinzetshuNo ratings yet
- Vitamin DDocument7 pagesVitamin DEirna Syam Fitri IINo ratings yet
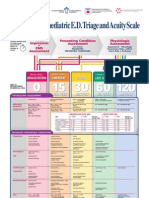
- Paediatric Triage PosterDocument1 pagePaediatric Triage PosterGenaro Olmos Garcia100% (2)
- Type 1 HypersensitivityDocument38 pagesType 1 Hypersensitivitychocoholic potchiNo ratings yet
- Respiratory SystemDocument104 pagesRespiratory SystemKatisha JosephNo ratings yet
- Psychosomatic Theory of Bronchia AsthmaDocument11 pagesPsychosomatic Theory of Bronchia AsthmaMaria RiveraNo ratings yet
- Bronchial Asthma PDFDocument32 pagesBronchial Asthma PDFArpitha YadavalliNo ratings yet
- Discharge Planning ASTHMADocument4 pagesDischarge Planning ASTHMANadja JamilahNo ratings yet
- Buteyko Breathing: What Is It?Document6 pagesButeyko Breathing: What Is It?Sundar Raj100% (1)
- Emergency Acupressure TreatmentDocument38 pagesEmergency Acupressure TreatmentEnergia de Cura100% (3)
- Klasifikasi Asma Gina 2015Document34 pagesKlasifikasi Asma Gina 2015Roni Ardian100% (1)
- Leaflet Bricanyl TurbohalerDocument7 pagesLeaflet Bricanyl TurbohalerKrisna SyammaNo ratings yet
- English Short Stories For Beginners and Intermediate LearnersDocument79 pagesEnglish Short Stories For Beginners and Intermediate LearnersVitor Vasconcelos100% (3)
- Professional PortfolioDocument2 pagesProfessional Portfolioapi-514966812No ratings yet
- BIOC3364 - 2021 Lecture Notes AsthmaDocument26 pagesBIOC3364 - 2021 Lecture Notes AsthmachrystalNo ratings yet
- Effectiveness of Nebulised Salbutamol Administered in Ambulances To Patients With Severe Acute AsthmaDocument4 pagesEffectiveness of Nebulised Salbutamol Administered in Ambulances To Patients With Severe Acute AsthmaMaria ClaraNo ratings yet
- Faktor Risiko AsmaDocument8 pagesFaktor Risiko AsmaAbdusSomadNo ratings yet
- SymbicortDocument18 pagesSymbicortkaditasookdeoNo ratings yet
- Pulmonology: The Cells of The Bronchial Epithelium, LeucocytesDocument64 pagesPulmonology: The Cells of The Bronchial Epithelium, LeucocytesSk Chaudhry100% (1)
- Rational Drug Therapy For The Management of Asthma Disease at MMCTH, MardanDocument118 pagesRational Drug Therapy For The Management of Asthma Disease at MMCTH, MardanDr. Salman Khan100% (1)
- Argumentative EssayDocument9 pagesArgumentative Essayapi-412321892No ratings yet
- Common Health Problems of Infancy PowptDocument78 pagesCommon Health Problems of Infancy PowptCiella Dela CruzNo ratings yet
- Asthma PDFDocument22 pagesAsthma PDFمحمد علي حريج / مسائيNo ratings yet
- Smolensky-Chronobiology and Chronotherapy of Allergic Rhinitis and Bronchial AsthmaDocument31 pagesSmolensky-Chronobiology and Chronotherapy of Allergic Rhinitis and Bronchial Asthmaeva yustianaNo ratings yet
- Dr. Rishi Pal: Asstt. ProfessorDocument40 pagesDr. Rishi Pal: Asstt. ProfessortamaNo ratings yet
- Unit Test - Fourth QuarterDocument2 pagesUnit Test - Fourth QuartergretchelleNo ratings yet
- Pharmacology Drug CardsDocument33 pagesPharmacology Drug CardssuedayrobinsonNo ratings yet
- Key Changes Gold 2023 2Document16 pagesKey Changes Gold 2023 2Muhammad Nur Ardhi LahabuNo ratings yet
- Bronchial Asthma & Cardiac AsthmaDocument7 pagesBronchial Asthma & Cardiac AsthmaAbraham Chiu100% (1)
- Ganesha MudraDocument146 pagesGanesha MudramamedeiaNo ratings yet
- Asthma Case Study.Document6 pagesAsthma Case Study.sammyNo ratings yet
- Páginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Document1 pagePáginas Desde A Stepwise Approach To The Interpretation of Pulmonary Function Tests-1Sotfonic SotfonicNo ratings yet