You might also like
- How To ForgiveDocument3 pagesHow To ForgiveAnonymous 0PYZofvGSNo ratings yet
- Electronic Circuits, Transformerless Power Supply, LED Drivers, Battery Chargers, Solar Circuits - Automatic Simple 12V 100ma NiCd Battery Charger Circuit PDFDocument2 pagesElectronic Circuits, Transformerless Power Supply, LED Drivers, Battery Chargers, Solar Circuits - Automatic Simple 12V 100ma NiCd Battery Charger Circuit PDFdewasuryanto100% (1)
- Electronic Circuits, Transformerless Power Supply, LED Drivers, Battery Chargers, Solar Circuits - Automatic Simple 12V 100ma NiCd Battery Charger Circuit PDFDocument2 pagesElectronic Circuits, Transformerless Power Supply, LED Drivers, Battery Chargers, Solar Circuits - Automatic Simple 12V 100ma NiCd Battery Charger Circuit PDFdewasuryanto100% (1)
- Herbal GuideDocument42 pagesHerbal GuideladygreenNo ratings yet
- SNR Englisch-3Document6 pagesSNR Englisch-3Geoff WhiteNo ratings yet
- Modern Trends in Hypnosis Ed by David Waxman & Prem C Misra & Michael Gibson & M Anthony Basker (1985)Document404 pagesModern Trends in Hypnosis Ed by David Waxman & Prem C Misra & Michael Gibson & M Anthony Basker (1985)marcinlesniewicz100% (4)
- Healing WonderDocument31 pagesHealing WonderRussiel DagohoyNo ratings yet
- home-delhimed-downloadfile-IMA NATCON SCIENTIFIC PROGRAME PDFDocument15 pageshome-delhimed-downloadfile-IMA NATCON SCIENTIFIC PROGRAME PDFRaveenaNo ratings yet
- Scapula Setting AnaIsabel AlmeidaDocument1 pageScapula Setting AnaIsabel AlmeidaPeter ZachNo ratings yet
- High-Range Wireless PowerDocument14 pagesHigh-Range Wireless PowerdewasuryantoNo ratings yet
- Internet Addiction INFODocument3 pagesInternet Addiction INFOstuti jainNo ratings yet
- Kuliah Ante Natal Care DR Dhanasari UIDocument21 pagesKuliah Ante Natal Care DR Dhanasari UIdewasuryantoNo ratings yet
- Battery ChargerDocument5 pagesBattery ChargerdewasuryantoNo ratings yet
- 12V Gelled-Electrolyte Battery ChargerDocument2 pages12V Gelled-Electrolyte Battery ChargerdewasuryantoNo ratings yet
- The Case of Dora and Her DreamsDocument5 pagesThe Case of Dora and Her DreamsHardik Motsara100% (1)
- Current Activated Switch - DIYWikiDocument5 pagesCurrent Activated Switch - DIYWikidewasuryantoNo ratings yet
- NCP - Acute PainDocument3 pagesNCP - Acute PainRoxanne NavarroNo ratings yet
- Automatic Water Tank Level Controller With Dry Pump Run Protection Using ArduinoDocument17 pagesAutomatic Water Tank Level Controller With Dry Pump Run Protection Using Arduinodewasuryanto100% (1)
- Ijhbr January 2018 23-30Document8 pagesIjhbr January 2018 23-30farhanomeNo ratings yet
- Deep Venous Thrombosis After Percutaneous Insertion of Vena Caval FiltersDocument9 pagesDeep Venous Thrombosis After Percutaneous Insertion of Vena Caval Filtersari kurniawanNo ratings yet
- Ijvm2014 531689 PDFDocument6 pagesIjvm2014 531689 PDFReka HariskianaNo ratings yet
- Jurnal VaskularDocument5 pagesJurnal VaskulardrelvNo ratings yet
- Tugas Praktikum SpssDocument2 pagesTugas Praktikum SpssjunNo ratings yet
- Deep Vein Thrombosis (DVT) Is A Precursor of Potentially Fatal PulmonaryDocument4 pagesDeep Vein Thrombosis (DVT) Is A Precursor of Potentially Fatal PulmonaryHatem ShafelNo ratings yet
- Early Follow-Up and Treatment Recommendations For Isolated Calf Deep Venous ThrombosisDocument5 pagesEarly Follow-Up and Treatment Recommendations For Isolated Calf Deep Venous ThrombosisDr. Aditya ShindeNo ratings yet
- The Importance of Monophasic Doppler Waveforms in The Common Femoral VeinDocument7 pagesThe Importance of Monophasic Doppler Waveforms in The Common Femoral Veindgina8800No ratings yet
- LnnkomplikacijeDocument8 pagesLnnkomplikacijeVinko GrubišićNo ratings yet
- Detection of Unsuspected Pelvic Dvts On Abdominopelvic CT Scans: A Potentially Life-Saving DiagnosisDocument5 pagesDetection of Unsuspected Pelvic Dvts On Abdominopelvic CT Scans: A Potentially Life-Saving DiagnosisKumail KhandwalaNo ratings yet
- 2014 - Jonathan Caronia - Residentperformedtwopointcompressionultrasoundisin (Retrieved-2015!10!13)Document5 pages2014 - Jonathan Caronia - Residentperformedtwopointcompressionultrasoundisin (Retrieved-2015!10!13)Ali MullaNo ratings yet
- Venous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesDocument13 pagesVenous Thromboembolism in Patients Discharged From The Emergency Department With Ankle FracturesSebastiano Della CasaNo ratings yet
- 2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathyDocument9 pages2000 - Stamm Et Al. - Surgery For Bilateral Outflow Tract Obstruction in Elastin ArteriopathybanupluNo ratings yet
- Dutta 2017Document3 pagesDutta 2017Kartik DuttaNo ratings yet
- JHM 2112Document4 pagesJHM 2112senkonenNo ratings yet
- 1 s2.0 S0378603X14001053 MainDocument10 pages1 s2.0 S0378603X14001053 MainAdrian PachecoNo ratings yet
- DVT in India PDFDocument6 pagesDVT in India PDFKarthik KoneruNo ratings yet
- Arenas-Jiménez2000 Article EvaluationOfCTFindingsForDiagnDocument10 pagesArenas-Jiménez2000 Article EvaluationOfCTFindingsForDiagnJulieta RGNo ratings yet
- Guidelines On Travel-Related Venous Thrombosis: GuidelineDocument4 pagesGuidelines On Travel-Related Venous Thrombosis: GuidelineNourhan JamalNo ratings yet
- Deep Venous Thrombosis Diferential DiagnosisDocument8 pagesDeep Venous Thrombosis Diferential DiagnosisBeby Dwi Lestari BajryNo ratings yet
- Fluid Complications: Malignant Pleural EffusionDocument11 pagesFluid Complications: Malignant Pleural Effusiont4tranNo ratings yet
- Computer-Assisted Transcatheter Heart Valve Implantation in Valve-in-Valve ProceduresDocument8 pagesComputer-Assisted Transcatheter Heart Valve Implantation in Valve-in-Valve ProceduresrédaNo ratings yet
- Jurnal VaskularDocument5 pagesJurnal VaskulardrelvNo ratings yet
- Wetenschappelijk ArtikelDocument7 pagesWetenschappelijk Artikel5rfffgfgNo ratings yet
- 2137 FullDocument7 pages2137 FullCourtneykdNo ratings yet
- 5 Sagban2015Document7 pages5 Sagban2015mihaelamocanNo ratings yet
- Hemoptisis 1Document11 pagesHemoptisis 1habiba rositaNo ratings yet
- Fibrinolysis Shutdown Correlation With Thromboembolic Events in Severe COVID-19 InfectionDocument12 pagesFibrinolysis Shutdown Correlation With Thromboembolic Events in Severe COVID-19 InfectionRia GandaNo ratings yet
- Diagnostic Assessment BeforeDocument4 pagesDiagnostic Assessment BeforeBinod KumarNo ratings yet
- Deep Vein Thrombosis in Stroke Patients:: Eulogio R. SiosonDocument6 pagesDeep Vein Thrombosis in Stroke Patients:: Eulogio R. SiosonDianti SuryonoNo ratings yet
- Pan Nucci 2011Document8 pagesPan Nucci 2011Ana I. NevarezNo ratings yet
- Diagnosis of Deep Venous Thrombosis and Pulmonary EmbolismDocument7 pagesDiagnosis of Deep Venous Thrombosis and Pulmonary EmbolismNataly VanesaNo ratings yet
- Transcatheter Coil Embolotherapy: A Safe and Evective Option For Major Colonic HaemorrhageDocument7 pagesTranscatheter Coil Embolotherapy: A Safe and Evective Option For Major Colonic Haemorrhagemuhammad gagas sasongkoNo ratings yet
- Blom JW - Malignancies, Prothrombotic Mutations, and The Risk of Venous ThrombosisDocument8 pagesBlom JW - Malignancies, Prothrombotic Mutations, and The Risk of Venous ThrombosisFarid RakhmanNo ratings yet
- 6514 23132 1 PBDocument3 pages6514 23132 1 PBdewminiNo ratings yet
- Prospective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsDocument5 pagesProspective Evaluation of Factors Associated With Early Failure of Arteriovenous Fistulae in Hemodialysis PatientsIvor WilopoNo ratings yet
- Pulmonary EmbolismDocument53 pagesPulmonary EmbolismSultan Al-rabeahNo ratings yet
- Deep Venous Thrombosis After Orthopedic PDFDocument7 pagesDeep Venous Thrombosis After Orthopedic PDFAnh Nguyen HuuNo ratings yet
- Mav-Vascularização Miometrial - 2020Document7 pagesMav-Vascularização Miometrial - 2020joaogualda19No ratings yet
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDocument9 pagesSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNo ratings yet
- Pinch Off Syndrome - A Rare Complication of Chemo Port: Dr. C. Ramachandra, Dr. Pavan Kumar J, Dr. C. SrinivasDocument4 pagesPinch Off Syndrome - A Rare Complication of Chemo Port: Dr. C. Ramachandra, Dr. Pavan Kumar J, Dr. C. SrinivasPavan JonnadaNo ratings yet
- Embolization in The Management of Recurrent Secondary Post-Tonsillectomy Haemorrhage in ChildrenDocument7 pagesEmbolization in The Management of Recurrent Secondary Post-Tonsillectomy Haemorrhage in ChildrenNicolás HenaoNo ratings yet
- Derrame PleuralDocument8 pagesDerrame PleuralFelipeNo ratings yet
- Etiologies of Bilateral Pleural EffusionsDocument8 pagesEtiologies of Bilateral Pleural EffusionsAlexander Lukky SugondoNo ratings yet
- Increased Minimum Vein Diameter On PreoperativeDocument40 pagesIncreased Minimum Vein Diameter On PreoperativeMikael AngelooNo ratings yet
- Jurnal THTDocument3 pagesJurnal THTValentina AdindaNo ratings yet
- HSHDDocument193 pagesHSHDRianda AkmalNo ratings yet
- A 40 YearsDocument9 pagesA 40 YearsDra Mariana Huerta CampaNo ratings yet
- Artigo 3Document7 pagesArtigo 3Lucas SantosNo ratings yet
- Radial Artery Access For Peripheral Endovascular ProceduresDocument6 pagesRadial Artery Access For Peripheral Endovascular Proceduresvam buddhaNo ratings yet
- Thromboprohylaxis and DVT in Surgical PRDocument7 pagesThromboprohylaxis and DVT in Surgical PRAhmed MohammedNo ratings yet
- Primary and Staged Transposition Arteriovenous Fistulas (Superficialization)Document5 pagesPrimary and Staged Transposition Arteriovenous Fistulas (Superficialization)Anonymous LnWIBo1GNo ratings yet
- Value of Red Blood Cell Distribution Width On Emergency Department Admission in Patients With Venous ThrombosisDocument6 pagesValue of Red Blood Cell Distribution Width On Emergency Department Admission in Patients With Venous ThrombosisJicko Street HooligansNo ratings yet
- Doipdf10 11771358863X10391355Document9 pagesDoipdf10 11771358863X10391355g2rpt6nzvnNo ratings yet
- Deep Venous Thrombosis After Total Joint ArthroplastyDocument7 pagesDeep Venous Thrombosis After Total Joint ArthroplastyJesse CusterNo ratings yet
- Chandra 2013Document5 pagesChandra 2013Jose YoveraNo ratings yet
- First-Line Arteriovenous Access and Risks of Hospitalization and Death in Patients Starting Hemodialysis - A Nationwide Cohort StudyDocument34 pagesFirst-Line Arteriovenous Access and Risks of Hospitalization and Death in Patients Starting Hemodialysis - A Nationwide Cohort StudyJimenez-Espinosa JeffersonNo ratings yet
- Complications Associated With Ivanissevich PDFDocument3 pagesComplications Associated With Ivanissevich PDFTahir TahirNo ratings yet
- Transcatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsFrom EverandTranscatheter Aortic Valve Replacement: A How-to Guide for Cardiologists and Cardiac SurgeonsNo ratings yet
- Phlebology, Vein Surgery and Ultrasonography: Diagnosis and Management of Venous DiseaseFrom EverandPhlebology, Vein Surgery and Ultrasonography: Diagnosis and Management of Venous DiseaseNo ratings yet
- Kimax HD03WF Product User Manual Hd03wfDocument16 pagesKimax HD03WF Product User Manual Hd03wfdewasuryantoNo ratings yet
- Simple Ultrasonic Range Finder Using Arduino. Circuit Diagram, Program and TheoryDocument4 pagesSimple Ultrasonic Range Finder Using Arduino. Circuit Diagram, Program and Theorydewasuryanto100% (1)
- Distance Measurement Using Arduino Ultrasonic Sensor - Code & Circuit DiagramDocument6 pagesDistance Measurement Using Arduino Ultrasonic Sensor - Code & Circuit DiagramdewasuryantoNo ratings yet
- Smart Blind Stick Project Using Arduino and SensorsDocument11 pagesSmart Blind Stick Project Using Arduino and SensorsdewasuryantoNo ratings yet
- Jurnal CovidDocument6 pagesJurnal CovidHanif MiftahNo ratings yet
- How To Build NiCd Battery Charger With Reverse Polarity ProtectionDocument1 pageHow To Build NiCd Battery Charger With Reverse Polarity ProtectiondewasuryantoNo ratings yet
- Water Level Controller Using Arduino. Water Level Indicator Using ArduinoDocument3 pagesWater Level Controller Using Arduino. Water Level Indicator Using Arduinodewasuryanto0% (1)
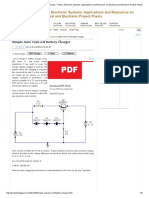
- Simple Auto Turn-Off Battery ChargerDocument5 pagesSimple Auto Turn-Off Battery ChargerdewasuryantoNo ratings yet
- Simple NiCd Battery ChargerDocument2 pagesSimple NiCd Battery Chargerdewasuryanto100% (1)
- Building A Smart Master - Slave SwitchDocument4 pagesBuilding A Smart Master - Slave SwitchdewasuryantoNo ratings yet
- Water Level Indicator Using Arduino & Ultrasonic Sensor - Circuit, ProgramDocument8 pagesWater Level Indicator Using Arduino & Ultrasonic Sensor - Circuit, ProgramdewasuryantoNo ratings yet
- NiMh and NiCd Battery Charger Circuit Circuit Diagram and InstructionsDocument1 pageNiMh and NiCd Battery Charger Circuit Circuit Diagram and InstructionsdewasuryantoNo ratings yet
- Mains Slave Switcher - DIYDocument2 pagesMains Slave Switcher - DIYdewasuryantoNo ratings yet
- K193 - Smart SLA Battery ChargerDocument3 pagesK193 - Smart SLA Battery ChargerdewasuryantoNo ratings yet
- Automatic NiCd Battery Charger CircuitDocument2 pagesAutomatic NiCd Battery Charger CircuitdewasuryantoNo ratings yet
- KUBE Electronics AG - Smart SwitchDocument2 pagesKUBE Electronics AG - Smart SwitchdewasuryantoNo ratings yet
- File - Current Sensor Circuit - PNG DIYWikiDocument1 pageFile - Current Sensor Circuit - PNG DIYWikidewasuryanto100% (1)
- Master Slave SwitcherDocument1 pageMaster Slave SwitcherdewasuryantoNo ratings yet
- Automatic Load Sensing Power Switch - EEWeb CommunityDocument2 pagesAutomatic Load Sensing Power Switch - EEWeb CommunitydewasuryantoNo ratings yet
- Automatic Switch For Voltage Converters Circuit DiagramDocument2 pagesAutomatic Switch For Voltage Converters Circuit DiagramdewasuryantoNo ratings yet
- Mains Slave TriacDocument2 pagesMains Slave Triacdewasuryanto100% (3)
- Dimmer Circuit Using SCR - TRIACDocument10 pagesDimmer Circuit Using SCR - TRIACdewasuryantoNo ratings yet
- Hypokalemic Periodic ParalysisDocument2 pagesHypokalemic Periodic ParalysissakuraleeshaoranNo ratings yet
- Stainless Steel Crown in Clinical Pedodontics - A ReviewDocument5 pagesStainless Steel Crown in Clinical Pedodontics - A ReviewmztahuNo ratings yet
- Hyperosmolar Hyperglycemic State (HHS)Document21 pagesHyperosmolar Hyperglycemic State (HHS)Malueth AnguiNo ratings yet
- Criterios de Elegibilidad de ACODocument88 pagesCriterios de Elegibilidad de ACOquimegiNo ratings yet
- 06 Senior Citizen PolicyDocument26 pages06 Senior Citizen PolicyJaimson FrancisNo ratings yet
- Tutorial Assignment Week 14 With AnswerDocument4 pagesTutorial Assignment Week 14 With AnswerCik Wynn100% (1)
- Introduction Definition: Types of PacemakersDocument8 pagesIntroduction Definition: Types of PacemakersPrasann RoyNo ratings yet
- (FEU) Central Venous Pressure Notes PDFDocument25 pages(FEU) Central Venous Pressure Notes PDFBryJos tiongsonNo ratings yet
- Antibiotic Guidelines For BONE AND JOINT INFECTIONSDocument3 pagesAntibiotic Guidelines For BONE AND JOINT INFECTIONSKhurram NadeemNo ratings yet
- OT and Eating DysfunctionDocument1 pageOT and Eating DysfunctionMCris EsSemNo ratings yet
- Dorothea Orem-Self Care TheoryDocument10 pagesDorothea Orem-Self Care TheoryNikhil MohanNo ratings yet
- Health As Expanding ConsciousnessDocument8 pagesHealth As Expanding ConsciousnessJun ManNo ratings yet
- NRSG - Documentation and Quality Management in IvtDocument12 pagesNRSG - Documentation and Quality Management in IvtRamon Carlo AlmiranezNo ratings yet
- Case Study 2Document6 pagesCase Study 2Gertie Mae CuicoNo ratings yet
- ASEAN Guideline On Stability of Drug ProductDocument8 pagesASEAN Guideline On Stability of Drug ProductSanjiv MenonNo ratings yet
- Vadney Resume 2Document2 pagesVadney Resume 2api-251597905No ratings yet
- PHD Thesis Ram Dheeraj Business Admin PDFDocument292 pagesPHD Thesis Ram Dheeraj Business Admin PDFplaycharles89No ratings yet
- RRL Anne)Document27 pagesRRL Anne)api-3728522No ratings yet
- Chapter 1 Developmental Disorders of The Oral CavityDocument6 pagesChapter 1 Developmental Disorders of The Oral CavityArafat Masud NiloyNo ratings yet
- Equipos Monitoreo de CondicionesDocument11 pagesEquipos Monitoreo de CondicionesJonathan Vasquez LlagunoNo ratings yet