You might also like
- Chapter 4Document7 pagesChapter 4jess forfodNo ratings yet
- Appendix 3: GRADE Evidence Profile ExamplesDocument1 pageAppendix 3: GRADE Evidence Profile ExamplesthelordhaniNo ratings yet
- Dealing with Data: The Commonwealth and International Library: Physics DivisionFrom EverandDealing with Data: The Commonwealth and International Library: Physics DivisionRating: 5 out of 5 stars5/5 (1)
- EBM presentation review key definitions and forest plotsDocument6 pagesEBM presentation review key definitions and forest plotssabrinaNo ratings yet
- Worksheet Summary FindingsDocument2 pagesWorksheet Summary FindingsLenie OdianNo ratings yet
- Optimal Management of Anticoagulation Therapy: An Educational Slide SetDocument43 pagesOptimal Management of Anticoagulation Therapy: An Educational Slide SetHNINNo ratings yet
- Assessment of Qualitative Test Performance and UncertaintyDocument15 pagesAssessment of Qualitative Test Performance and UncertaintyPaulo PereiraNo ratings yet
- Ecological Cross-Sectional Case-Control Cohort Randomised Controlled Trials (RCTS) Systematic Reviews Meta-AnalysesDocument3 pagesEcological Cross-Sectional Case-Control Cohort Randomised Controlled Trials (RCTS) Systematic Reviews Meta-AnalysesPetros SkapinakisNo ratings yet
- New Uhb StatisticsDocument33 pagesNew Uhb StatisticsTri YustiNo ratings yet
- Venous Thromboembolism Prophylaxis in Orthopedic SurgeryDocument30 pagesVenous Thromboembolism Prophylaxis in Orthopedic SurgerymohNo ratings yet
- Manchester Triage System Global Standard for Emergency Department TriageDocument41 pagesManchester Triage System Global Standard for Emergency Department Triageeman sulaimanNo ratings yet
- Quality Control - CHEMISTRYDocument3 pagesQuality Control - CHEMISTRYAllyssa AniNo ratings yet
- Ajg 2021 04 06 Jaine Ajg-20-3275 sdc1Document43 pagesAjg 2021 04 06 Jaine Ajg-20-3275 sdc1Diego Armando Huaman VicenteNo ratings yet
- ARIA 2016 Evidence on Combination Therapy vs. Intranasal Corticosteroid AloneDocument76 pagesARIA 2016 Evidence on Combination Therapy vs. Intranasal Corticosteroid AloneKhandar YosuaNo ratings yet
- WHO RHR 11.10 EngDocument121 pagesWHO RHR 11.10 EngSven OrdanzaNo ratings yet
- Analysis of Clinical Trials Data and ResultsDocument18 pagesAnalysis of Clinical Trials Data and ResultsAshley WatsonNo ratings yet
- Gark - Stereotactic Radiosurgery For Spinal LesionsDocument66 pagesGark - Stereotactic Radiosurgery For Spinal LesionsÖzgür Kara (OncoHealth)No ratings yet
- Borderline ScreeningDocument3 pagesBorderline ScreeningAlexandreDuarteGiganteNo ratings yet
- Pengetahuan: Case Processing SummaryDocument4 pagesPengetahuan: Case Processing Summarydiah puspitasariNo ratings yet
- RCT Report - ChuaDocument36 pagesRCT Report - Chuanv5yy5ryd5No ratings yet
- Basic Study Designs for Medical ResearchDocument4 pagesBasic Study Designs for Medical ResearchJinah HwinnNo ratings yet
- Southeastern Regional Medical Center 2011-12 IPC Risk AssessmentDocument27 pagesSoutheastern Regional Medical Center 2011-12 IPC Risk AssessmentMOHAMEDNo ratings yet
- (CPG) Philippine Periodic Health Examination Phase 1 - Evidence SummariesDocument159 pages(CPG) Philippine Periodic Health Examination Phase 1 - Evidence SummariesKaren Mae PadillaNo ratings yet
- RCT DESIGN: RANDOMIZATION AND BLINDINGDocument40 pagesRCT DESIGN: RANDOMIZATION AND BLINDINGSheila Tirta AyumurtiNo ratings yet
- Nama: Riris Putri Marito Sinaga NIM: 04022722125001 Prodi: Ilmu Kesehatan Anak No Soal 35Document13 pagesNama: Riris Putri Marito Sinaga NIM: 04022722125001 Prodi: Ilmu Kesehatan Anak No Soal 35Riris SinagaNo ratings yet
- Acne Scars Pathogenesis Classification and TreatmentDocument10 pagesAcne Scars Pathogenesis Classification and TreatmentSpica AdharaNo ratings yet
- Prognostic Implication of 21-Gene Expression Assay in Luminal B Type Hormone Receptor-Positive Breast Cancer Patients Younger Than 40 YearsDocument9 pagesPrognostic Implication of 21-Gene Expression Assay in Luminal B Type Hormone Receptor-Positive Breast Cancer Patients Younger Than 40 Yearshoctiengphap2024No ratings yet
- CCM 46 9 2018 06 08 Devlin Ccmed-D-18-00069 sdc15Document47 pagesCCM 46 9 2018 06 08 Devlin Ccmed-D-18-00069 sdc15CarlosNo ratings yet
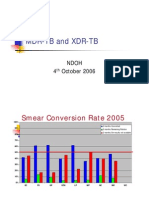
- MDR-TB and XDR-TB: Ndoh 4 October 2006Document40 pagesMDR-TB and XDR-TB: Ndoh 4 October 2006Eta Calvin ObenNo ratings yet
- Ercpvsptc Poster KK 4.23.2019Document1 pageErcpvsptc Poster KK 4.23.2019karan kauraNo ratings yet
- Facility-Onset Infections(s) Device-Or Care-Related: Clostridioides DifficileDocument2 pagesFacility-Onset Infections(s) Device-Or Care-Related: Clostridioides DifficileHeba HanyNo ratings yet
- Non InferiorityDocument10 pagesNon InferiorityproudofskyNo ratings yet
- Therapy Worksheet (Page 1 of 2) : A. VALIDITY: Are The Results of This Single Preventive or Therapeutic Trial Valid?Document15 pagesTherapy Worksheet (Page 1 of 2) : A. VALIDITY: Are The Results of This Single Preventive or Therapeutic Trial Valid?andhikaNo ratings yet
- Hasil Analisis Data - Mortalitas HIVDocument27 pagesHasil Analisis Data - Mortalitas HIVRickgo VirgoNo ratings yet
- HACCP Control MeasuresDocument4 pagesHACCP Control MeasuresAishwary SamarthNo ratings yet
- Academic Emergency Medicine - 2021 - Gottlieb - Colchicine For Acute Gout-1Document2 pagesAcademic Emergency Medicine - 2021 - Gottlieb - Colchicine For Acute Gout-10543394806No ratings yet
- WP Contentuploads201805CABANA Trial Slides 05092018FINAL PDFDocument19 pagesWP Contentuploads201805CABANA Trial Slides 05092018FINAL PDFJjawo GinesNo ratings yet
- Copd 2022Document20 pagesCopd 2022Abin PNo ratings yet
- Tarifbestimmungen Des WestfalenTarifsDocument23 pagesTarifbestimmungen Des WestfalenTarifsdiderotulNo ratings yet
- Eze Chidiebere 0207Document27 pagesEze Chidiebere 0207api-404356063No ratings yet
- Therapy Worksheet (Page 1 ofDocument9 pagesTherapy Worksheet (Page 1 ofNararyasri HoeseinNo ratings yet
- ISPE CTU Evaluation PresentationDocument25 pagesISPE CTU Evaluation PresentationOscar HoyosNo ratings yet
- EBM Multiple Choice QuestionsDocument2 pagesEBM Multiple Choice QuestionsDelelegn EmwodewNo ratings yet
- CriticalDocument10 pagesCriticalAisya FikritamaNo ratings yet
- Clinical Outcomes With Newer Antihyperglycemic Agents: FDA-Mandated CV Safety TrialsDocument27 pagesClinical Outcomes With Newer Antihyperglycemic Agents: FDA-Mandated CV Safety TrialsMohammed HammedNo ratings yet
- 400pmET Transcatheter Tricuspid Valve Treatment TCT 2019Document22 pages400pmET Transcatheter Tricuspid Valve Treatment TCT 2019KushanNo ratings yet
- Differences Between Case Control Cohort Cros SectionalDocument2 pagesDifferences Between Case Control Cohort Cros SectionalPriyanka ChinthapalliNo ratings yet
- Biostat Finals RevisedDocument3 pagesBiostat Finals Revisednnnn hhhhNo ratings yet
- BMJ 2023 076305.fullDocument11 pagesBMJ 2023 076305.fullcimongimutgemesNo ratings yet
- Cohort Design - Issues in Analysis - Overview2020Document16 pagesCohort Design - Issues in Analysis - Overview2020Monique ChaayaNo ratings yet
- CV TestsDocument1 pageCV TestsHarryNo ratings yet
- Updated Hypertension GuidelineDocument88 pagesUpdated Hypertension Guidelinekenny631653No ratings yet
- 2119 Manuscript 8588 1 10 20181026Document4 pages2119 Manuscript 8588 1 10 20181026Diannesa April GolosindaNo ratings yet
- 3 CC Must knowDocument27 pages3 CC Must knowSheena BlonesNo ratings yet
- Derezende 2020Document2 pagesDerezende 2020Pulmonologi Dan Kedokteran Respirasi FK UNRINo ratings yet
- IC Risk Assessment 2018 New FormDocument3 pagesIC Risk Assessment 2018 New FormBasma AzazNo ratings yet
- Perianal Condyloma Acuminata: Factors That Contribute To The RecurrenceDocument3 pagesPerianal Condyloma Acuminata: Factors That Contribute To The RecurrencetaagrettaaNo ratings yet
- SSRN Id3550054Document23 pagesSSRN Id3550054Oscar CastañedaNo ratings yet
- Low Flow and Minimalflow WP 999 en PDFDocument5 pagesLow Flow and Minimalflow WP 999 en PDFMica MariaNo ratings yet
- 10 1164@rccm 201703-0548ST-1Document11 pages10 1164@rccm 201703-0548ST-1dogui0071No ratings yet
- Cardiac Output Monitoring PDFDocument8 pagesCardiac Output Monitoring PDFMica MariaNo ratings yet
- Guidelines for managing acute respiratory distress syndromeDocument20 pagesGuidelines for managing acute respiratory distress syndromeMica MariaNo ratings yet
- AMRI Hospital TariffDocument42 pagesAMRI Hospital TariffsandeepNo ratings yet
- Dimension EXL 200/EXL With LM Integrated Chemistry Systems: Global Test MenuDocument2 pagesDimension EXL 200/EXL With LM Integrated Chemistry Systems: Global Test MenuGuneyden GuneydenNo ratings yet
- DNB QUESTION PAPER-Topic Wise (Author DR - Sirisha)Document92 pagesDNB QUESTION PAPER-Topic Wise (Author DR - Sirisha)Sirisha CkvNo ratings yet
- Case Presentation Hepatitis A LuluDocument28 pagesCase Presentation Hepatitis A LuluBrenda KarinaNo ratings yet
- Ultrasound-Guided Brachial Plexus BlockDocument7 pagesUltrasound-Guided Brachial Plexus BlockÇağdaş BaytarNo ratings yet
- Chapter 10 - Immune Responses Against Tumors and TransplantsDocument11 pagesChapter 10 - Immune Responses Against Tumors and TransplantsFYMNo ratings yet
- Cam4 5 1239Document12 pagesCam4 5 1239kadiksuhNo ratings yet
- TeresaDocument2 pagesTeresaapi-435131948No ratings yet
- Petrus Nnolim CVDocument5 pagesPetrus Nnolim CVagni.nnolimNo ratings yet
- FFT Neuroma Morton PDFDocument6 pagesFFT Neuroma Morton PDFdasamoroNo ratings yet
- Crystalloid and Colloid TherapyDocument11 pagesCrystalloid and Colloid TherapyAlexa UGNo ratings yet
- Petition To Remove James Wiley Conservator of The Estate of Henry C.MunozDocument2 pagesPetition To Remove James Wiley Conservator of The Estate of Henry C.MunozpropertylenderNo ratings yet
- Bronchoscopy: Dr. Ravi Gadani MS, FmasDocument17 pagesBronchoscopy: Dr. Ravi Gadani MS, FmasRaviNo ratings yet
- Supplement-1115 2020Document216 pagesSupplement-1115 2020Laura PaunicaNo ratings yet
- Consider Nursing School for a Fulfilling and In-Demand CareerDocument2 pagesConsider Nursing School for a Fulfilling and In-Demand CareerTangerine DianeNo ratings yet
- Shock and Hypoperfusion Mechanisms and TreatmentDocument46 pagesShock and Hypoperfusion Mechanisms and TreatmentIgor StefanetNo ratings yet
- Power Point Dr. ShintaDocument11 pagesPower Point Dr. ShintaAnonymous fOz6ToNo ratings yet
- Systemic in Ammatory Response Syndrome (SIRS) : Where Did It Come From and Is It Still Relevant Today?Document8 pagesSystemic in Ammatory Response Syndrome (SIRS) : Where Did It Come From and Is It Still Relevant Today?Jhanu JaguarNo ratings yet
- Psychosocial Aspect of Critical Nursing Pak JoDocument9 pagesPsychosocial Aspect of Critical Nursing Pak JoYuli Permata SARINo ratings yet
- Isicem 2021Document90 pagesIsicem 2021labbeneNo ratings yet
- Gavinos ResumeDocument4 pagesGavinos ResumeRI NANo ratings yet
- BPH PSPD 2012Document43 pagesBPH PSPD 2012Nor AinaNo ratings yet
- Lina Marulanda - Nursing Resume FinalDocument2 pagesLina Marulanda - Nursing Resume Finalapi-490969182No ratings yet
- Atrium MedicalDocument12 pagesAtrium MedicalBo TaoNo ratings yet
- Anorexia Nerviosa y Trastornos Del Espectro Autista Investigacion Guiada de Endofenotipos Cognitivos SocialesDocument31 pagesAnorexia Nerviosa y Trastornos Del Espectro Autista Investigacion Guiada de Endofenotipos Cognitivos SocialesCarito Hernandez RodriguezNo ratings yet
- Manual Procedure Hemoglobin Drabkin Colorimetric MethodDocument1 pageManual Procedure Hemoglobin Drabkin Colorimetric MethodAhmad SaeedNo ratings yet
- Ace InhibitorsDocument26 pagesAce InhibitorsDeipa KunwarNo ratings yet
- 1303miha OnePager01neutralDocument2 pages1303miha OnePager01neutralAlex YamilNo ratings yet
- 2016 - Byk FotoDocument7 pages2016 - Byk FotoSyifa IKNo ratings yet
- Aneroxia Research PaperDocument34 pagesAneroxia Research PaperDuaa HammadNo ratings yet