You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Pretreatment Diagnosis of Suprasellar Papillary Craniopharyngioma and Germ Cell Tumors of Adult PatientsDocument10 pagesPretreatment Diagnosis of Suprasellar Papillary Craniopharyngioma and Germ Cell Tumors of Adult PatientsTony Miguel Saba SabaNo ratings yet
- Individualizando Los Objetivos de TA en Diabéticos. de Boer I 2018.Document2 pagesIndividualizando Los Objetivos de TA en Diabéticos. de Boer I 2018.Tony Miguel Saba SabaNo ratings yet
- 2018 ESC-EACTS Guidelines On Myocardial RevascularizationDocument96 pages2018 ESC-EACTS Guidelines On Myocardial RevascularizationTony Miguel Saba SabaNo ratings yet
- Effectiveness and Safety of Carbohydrate Counting in The Management of Adult Patients With Type 1 Diabetes Mellitus A Systematic Review and Meta-AnalysisDocument9 pagesEffectiveness and Safety of Carbohydrate Counting in The Management of Adult Patients With Type 1 Diabetes Mellitus A Systematic Review and Meta-AnalysisTony Miguel Saba SabaNo ratings yet
- The Challenges of Restructuring Health Care in VenezuelaDocument2 pagesThe Challenges of Restructuring Health Care in VenezuelaFelix J. TapiaNo ratings yet
- Prioritising Risk Factors For Type 2 Diabetes Causal Inference Through Genetic ApproachesDocument10 pagesPrioritising Risk Factors For Type 2 Diabetes Causal Inference Through Genetic ApproachesTony Miguel Saba SabaNo ratings yet
- HIV Infection, Pulmonary Tuberculosis, and COPD in Rural Uganda A Cross-Sectional StudyDocument9 pagesHIV Infection, Pulmonary Tuberculosis, and COPD in Rural Uganda A Cross-Sectional StudyTony Miguel Saba SabaNo ratings yet
- Hipogonadismo MasculinoDocument2 pagesHipogonadismo MasculinoTony Miguel Saba SabaNo ratings yet
- The Α-cell in Diabetes MellitusDocument11 pagesThe Α-cell in Diabetes MellitusTony Miguel Saba SabaNo ratings yet
- Good, Bad, or Ugly The Biological Roles of Bone Marrow FatDocument8 pagesGood, Bad, or Ugly The Biological Roles of Bone Marrow FatTony Miguel Saba SabaNo ratings yet
- Evaluación y Manejo de Los Pólipos GástricosDocument7 pagesEvaluación y Manejo de Los Pólipos GástricosTony Miguel Saba SabaNo ratings yet
- Myocardial Infarction ESCDocument33 pagesMyocardial Infarction ESCddantoniusgmailNo ratings yet
- Conversion From Insulin Glargine U-100 To Insulin Glargine U-300 or Insulin Degludec and The Impact On Dosage RequirementsDocument9 pagesConversion From Insulin Glargine U-100 To Insulin Glargine U-300 or Insulin Degludec and The Impact On Dosage RequirementsTony Miguel Saba SabaNo ratings yet
- Does Family History of Obesity, Cardiovascular, and Metabolic Diseases Influence Onset and Severity of Childhood ObesityDocument6 pagesDoes Family History of Obesity, Cardiovascular, and Metabolic Diseases Influence Onset and Severity of Childhood ObesityTony Miguel Saba SabaNo ratings yet
- Disminucion de Lípidos en Sindrome Coronario Agudo. Nicholls S 2018Document2 pagesDisminucion de Lípidos en Sindrome Coronario Agudo. Nicholls S 2018Tony Miguel Saba SabaNo ratings yet
- For Patients With Type 2 Diabetes, What's The Best Target Hemoglobin A1CDocument2 pagesFor Patients With Type 2 Diabetes, What's The Best Target Hemoglobin A1CTony Miguel Saba SabaNo ratings yet
- Effects of Weight Loss On Acoustic Parameters After Bariatric SurgeryDocument2 pagesEffects of Weight Loss On Acoustic Parameters After Bariatric SurgeryTony Miguel Saba SabaNo ratings yet
- Thyroid Hormone Status in Patients With Severe Selenium DeficiencyDocument8 pagesThyroid Hormone Status in Patients With Severe Selenium DeficiencyTony Miguel Saba SabaNo ratings yet
- Effects of weight loss on voice after bariatric surgeryDocument5 pagesEffects of weight loss on voice after bariatric surgeryTony Miguel Saba SabaNo ratings yet
- Predictors of Success in Bariatric Surgery The Role of BMI and Pre-Operative ComorbiditiesDocument7 pagesPredictors of Success in Bariatric Surgery The Role of BMI and Pre-Operative ComorbiditiesTony Miguel Saba SabaNo ratings yet
- Elipse Balloon The Pitfalls of Excessive SimplicityDocument3 pagesElipse Balloon The Pitfalls of Excessive SimplicityTony Miguel Saba SabaNo ratings yet
- Literatura en La Web Asociada A Cirugía BariátricaDocument8 pagesLiteratura en La Web Asociada A Cirugía BariátricaTony Miguel Saba SabaNo ratings yet
- Bariatric Surgery As An Efficient Treatment For Non-Alcoholic Fatty Liver Disease in A Prospective Study With 1-Year Follow-UpDocument9 pagesBariatric Surgery As An Efficient Treatment For Non-Alcoholic Fatty Liver Disease in A Prospective Study With 1-Year Follow-UpTony Miguel Saba SabaNo ratings yet
- Elipse Balloon The Pitfalls of Excessive SimplicityDocument3 pagesElipse Balloon The Pitfalls of Excessive SimplicityTony Miguel Saba SabaNo ratings yet
- Effects of weight loss on voice after bariatric surgeryDocument5 pagesEffects of weight loss on voice after bariatric surgeryTony Miguel Saba SabaNo ratings yet
- Contraception, Menstruation, and Sexuality After Bariatric Surgery A Prospective Cohort StudyDocument9 pagesContraception, Menstruation, and Sexuality After Bariatric Surgery A Prospective Cohort StudyTony Miguel Saba SabaNo ratings yet
- One Anastomosis Gastric Bypass and Risk of CancerDocument4 pagesOne Anastomosis Gastric Bypass and Risk of CancerTony Miguel Saba SabaNo ratings yet
- Does Bariatric Surgery Affect The Incidence of Endometrial Cancer Development A Systematic ReviewDocument8 pagesDoes Bariatric Surgery Affect The Incidence of Endometrial Cancer Development A Systematic ReviewTony Miguel Saba SabaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Psychological First Aid-A Training GuideDocument8 pagesPsychological First Aid-A Training Guidejprewittdiaz100% (1)
- Proptosis UnilateralDocument5 pagesProptosis UnilateralCarlos NiveloNo ratings yet
- Facts About Penis SizeDocument5 pagesFacts About Penis Sizeabumadeh1423No ratings yet
- Evidence-Based Strategies For The Minimally Invasive Treatment of Carious Lesions: Review of The LiteratureDocument8 pagesEvidence-Based Strategies For The Minimally Invasive Treatment of Carious Lesions: Review of The LiteratureNaji Z. ArandiNo ratings yet
- Protocols Sepsis Treatment Stony BrookDocument6 pagesProtocols Sepsis Treatment Stony BrookVicky Chrystine SianiparNo ratings yet
- Occlusal Considerations for Removable Partial DenturesDocument15 pagesOcclusal Considerations for Removable Partial DenturesVikas AggarwalNo ratings yet
- The Differences Between Coaching Mentoring Therapy and Counselling PDFDocument5 pagesThe Differences Between Coaching Mentoring Therapy and Counselling PDFghinaNo ratings yet
- Cognitive Rehabilitation Programs in Schizophrenia PDFDocument26 pagesCognitive Rehabilitation Programs in Schizophrenia PDFMeindayaniNo ratings yet
- Sensory Deprivation and Loss-4Document32 pagesSensory Deprivation and Loss-4Scott Daniel Phillips100% (1)
- Psychoanalysis Case Study of Gregory HouseDocument6 pagesPsychoanalysis Case Study of Gregory HouseTheodora Catalina100% (2)
- Pharmacodynamics and Therapeutic Applications of Iboga and IbogaineDocument25 pagesPharmacodynamics and Therapeutic Applications of Iboga and IbogainejesterstableNo ratings yet
- Medsurg Cardio Ana&PhysioDocument6 pagesMedsurg Cardio Ana&Physiorabsibala80% (10)
- Avulsion and Degloving InjuryDocument12 pagesAvulsion and Degloving InjuryandicaNo ratings yet
- Anal FissuresDocument2 pagesAnal FissureskhadzxNo ratings yet
- PublicationDocument5 pagesPublicationMahfuzur RNo ratings yet
- Epworth Richmond - Agency Staff Orientation Booklet MAY 2016Document33 pagesEpworth Richmond - Agency Staff Orientation Booklet MAY 2016Anonymous BaD9jQNo ratings yet
- How I Provide A Paediatric Dysphagia Service (2) : Parents at The CentreDocument10 pagesHow I Provide A Paediatric Dysphagia Service (2) : Parents at The CentreSpeech & Language Therapy in PracticeNo ratings yet
- Endocrine SystemDocument25 pagesEndocrine Systemangel_maui100% (13)
- DPT Doctor of Physiotherapy Program at Abu Zafar InstituteDocument44 pagesDPT Doctor of Physiotherapy Program at Abu Zafar InstituteAbdul basit KaleemNo ratings yet
- Health Care Delivery System in IndiaDocument9 pagesHealth Care Delivery System in IndiaPrabhjot Singh100% (4)
- Reality Therapy: Charlene Raye C. TugadeDocument8 pagesReality Therapy: Charlene Raye C. TugadeCharlene Raye TugadeNo ratings yet
- NDT 45697 Efficacy of Second Generation Antipsychotics in Patients at 061813Document8 pagesNDT 45697 Efficacy of Second Generation Antipsychotics in Patients at 061813twahyuningsih_16No ratings yet
- #2&3 - 18 Street, West Bajac-Bajac, Olongapo City Telefax: (047) 6023200 Mobile: (+63) 920 9020591Document10 pages#2&3 - 18 Street, West Bajac-Bajac, Olongapo City Telefax: (047) 6023200 Mobile: (+63) 920 9020591Leo Arcillas Pacunio100% (1)
- ArthritisDocument15 pagesArthritisPrambudi KusumaNo ratings yet
- Patellofemoral Final PDFDocument12 pagesPatellofemoral Final PDFdvenumohanNo ratings yet
- Clinical Management in PsychodermatologyDocument294 pagesClinical Management in Psychodermatologymconsultorpsi100% (2)
- Beyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDDocument9 pagesBeyond The Manual: The Insider's Guide To Prolonged Exposure Therapy For PTSDmakolla007No ratings yet
- Intake AssessmentDocument2 pagesIntake Assessmentyourzxtruly0% (1)
- USUHS Anesthesia Pharmacology NotesetDocument247 pagesUSUHS Anesthesia Pharmacology NotesetSean Bancroft100% (3)
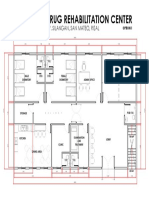
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet