Professional Documents
Culture Documents
2 Pag 4
Uploaded by
Mr. LOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
2 Pag 4
Uploaded by
Mr. LCopyright:
Available Formats
Articles
Drug-coated balloons for small coronary artery disease
(BASKET-SMALL 2): an open-label randomised
non-inferiority trial
Raban V Jeger, Ahmed Farah, Marc-Alexander Ohlow, Norman Mangner, Sven Möbius-Winkler, Gregor Leibundgut, Daniel Weilenmann,
Jochen Wöhrle, Stefan Richter, Matthias Schreiber, Felix Mahfoud, Axel Linke, Frank-Peter Stephan, Christian Mueller, Peter Rickenbacher,
Michael Coslovsky, Nicole Gilgen, Stefan Osswald, Christoph Kaiser, Bruno Scheller, for the BASKET-SMALL 2 Investigators
Summary
Background Drug-coated balloons (DCB) are a novel therapeutic strategy for small native coronary artery disease. Published Online
However, their safety and efficacy is poorly defined in comparison with drug-eluting stents (DES). August 28, 2018
http://dx.doi.org/10.1016/
S0140-6736(18)31719-7
Methods BASKET-SMALL 2 was a multicentre, open-label, randomised non-inferiority trial. 758 patients with de-
See Online/Comment
novo lesions (<3 mm in diameter) in coronary vessels and an indication for percutaneous coronary intervention were http://dx.doi.org/10.1016/
randomly allocated (1:1) to receive angioplasty with DCB versus implantation of a second-generation DES after S0140-6736(18)31926-3
successful predilatation via an interactive internet-based response system. Dual antiplatelet therapy was given University Hospital Basel,
according to current guidelines. The primary objective was to show non-inferiority of DCB versus DES regarding University of Basel, Basel,
Switzerland (Prof R V Jeger MD,
major adverse cardiac events (MACE; ie, cardiac death, non-fatal myocardial infarction, and target-vessel
F-P Stephan MD,
revascularisation) after 12 months. The non-inferiority margin was an absolute difference of 4% in MACE. This trial is Prof C Mueller MD,
registered with ClinicalTrials.gov, number NCT01574534. Prof P Rickenbacher MD,
M Coslovsky PhD, N Gilgen MD,
Prof S Osswald MD,
Findings Between April 10, 2012, and February 1, 2017, 382 patients were randomly assigned to the DCB group and
Prof C Kaiser MD);
376 to DES group. Non-inferiority of DCB versus DES was shown because the 95% CI of the absolute difference in Knappschaftskrankhenhaus,
MACE in the per-protocol population was below the predefined margin (–3·83 to 3·93%, p=0·0217). After 12 months, Klinikum Westfalen,
the proportions of MACE were similar in both groups of the full-analysis population (MACE was 7·5% for the DCB Dortmund, Germany
(A Farah MD); Central Clinic,
group vs 7·3% for the DES group; hazard ratio [HR] 0·97 [95% CI 0·58–1·64], p=0·9180). There were five (1·3%)
Bad Berka, Germany
cardiac-related deaths in the DES group and 12 (3·1%) in the DCB group (full analysis population). Probable or definite (Prof M-A Ohlow MD,
stent thrombosis (three [0·8%] in the DCB group vs four [1·1%] in the DES group; HR 0·73 [0·16–3·26]) and major S Richter MD, M Schreiber MD);
bleeding (four [1·1%] in the DCB group vs nine [2·4%] in the DES group; HR 0·45 [0·14–1·46]) were the most Herzzentrum Dresden,
Technische Universität
common adverse events. Dresden, Dresden, Germany
(N Mangner MD,
Interpretation In small native coronary artery disease, DCB was non-inferior to DES regarding MACE up to 12 months, Prof A Linke MD); Heart Center
with similar event rates for both treatment groups. Leipzig, University Hospital,
Leipzig, Germany (N Mangner,
Prof A Linke); University
Funding Schweizerischer Nationalfonds zur Förderung der Wissenschaftlichen Forschung, Basel Cardiovascular Hospital Jena, Jena, Germany
Research Foundation, and B Braun Medical AG. (S Möbius-Winkler MD);
Cantonal Hospital Baselland,
Liestal, Switzerland
Copyright © 2018 Elsevier Ltd. All rights reserved. (G Leibundgut MD); Cantonal
Hospital St Gallen, St Gallen,
Introduction essential, as outlined in recommend ations.10 The Switzerland
Second-generation drug-eluting stents (DES) are the feasibility of the technique in small-vessel coronary artery (D Weilenmann MD); University
Hospital Ulm, Ulm, Germany
preferred treatment for percutaneous coronary inter disease has been suggested in several pilot studies.11–16 (Prof J Wöhrle MD); and
vention (PCI) in coronary artery disease.1 However, the However, to our knowledge, a large randomised University Hospital Saarland,
efficacy of stents is restricted in small coronary arteries.2 trial comparing DCB with second-generation DES with Homburg, Germany
This limitation applies to bare metal stents (BMS)3 and clinical endpoints has not been done. (Prof F Mahfoud MD,
Prof B Scheller MD)
first-generation and second-generation DES.4 The Basel Kosten Effektivitäts Trial–Drug-Coated
Correspondence to:
Drug-coated balloons (DCB) are a novel concept for the Balloons versus Drug-eluting Stents in Small Vessel Prof Raban V Jeger, University
treatment of coronary artery disease and an established Interventions (BASKET-SMALL) 2 trial aimed to test the Hospital Basel, University of
therapeutic option for restenosis of BMS5,6 and DES.7,8 non-inferiority of DCB versus second-generation DES in Basel, Basel 4031, Switzerland
The technique is based on the fast delivery of highly small vessel coronary artery disease using a 12-month raban.jeger@usb.ch
lipophilic drugs to the vessel wall after single balloon composite clinical endpoint of major adverse cardiac
inflation with a specific matrix.9 To over come the events (MACE), consisting of cardiac death, non-fatal
limitations of elastic recoil and flow-limiting dissections myocardial infarction, and target vessel revascularisation
after balloon angioplasty, optimal lesion preparation is in a large all-comer population.
www.thelancet.com Published online August 28, 2018 http://dx.doi.org/10.1016/S0140-6736(18)31719-7 1
Articles
Research in context
Evidence before this study non-inferiority of DCB versus second-generation DES in the
Second-generation drug-eluting stents (DES) are the standard treatment of lesions in coronary arteries of less than 3 mm in
treatment for coronary artery disease. However, their efficacy is diameter regarding major adverse cardiac events at 12 months.
restricted in small coronary arteries because of increased event After successful predilatation of the lesion with a standard
rates compared with larger vessel sizes. Drug-coated balloons balloon, 758 patients were randomly assigned to one of the
(DCB) are an established treatment option for in-stent restenosis two treatment groups. The findings show that the use of DCB
in bare metal stents and DES, but there is scarce evidence about in small vessel coronary artery disease is safe if an acceptable
the efficacy and safety of DCB in native small coronary artery angiographic result can be obtained after successful
disease. Advantages of DCB include the potential for favourable predilatation.
vascular remodelling after angioplasty in the absence of a stent,
Implications of all the available evidence
the theoretical absence of any stent thrombosis, and the option
A stent-free treatment of coronary artery disease with DCB is
of shortening dual antiplatelet therapy to only 4 weeks. Besides
safe if an acceptable angiographic result can be obtained after
non-randomised data, only two small, randomised controlled
predilatation of the lesion. To date, the technique is restricted
trials have been done in this field, using angiographic endpoints
to small coronary arteries, but might be expanded to larger
and first-generation DES as comparators.
vessel sizes with future research.
Added value of this study
BASKET-SMALL 2 is a pivotal multicentre randomised
controlled study in a large all-comer population and shows the
Methods Randomisation and masking
Study design We used an interactive internet-based response system to
BASKET-SMALL 2 is an investigator-initiated, prospect randomly assign participants (1:1) to receive either
ive, randomised, multicentre, open-label, non-inferiority angioplasty with DCB or implantation of a second-
trial.17 The trial was done at 14 participating centres generation DES after successful predilatation.
See Online for appendix (appendix). The trial was done in accordance with the This trial was open-label; therefore, participants or
Declaration of Helsinki and Good Clinical Practice investigators were not masked to the treatment.
guidelines, and the protocol (appendix) was approved by
the ethics committees in all participating centres. Procedures
Participants in the DCB group received the paclitaxel-
Participants coated balloon SeQuent Please (B Braun Melsungen AG,
All patients with an indication for PCI either due to acute Melsungen, Germany), and those in the DES group
coronary syndrome, chronic angina pectoris, or silent received one of two second-generation DES: the
ischemia, and angiographic lesions in native coronary everolimus-eluting Xience stent (Abbott Vascular, Santa
arteries with a diameter of 2 mm to less than 3 mm were Clara, CA, USA) or the paclitaxel-eluting Taxus Element
eligible for enrolment. However, randomisation was only stent (Boston Scientific, Natick, MA, USA). The study
possible if predilatation of the lesion with an angioplasty was started with Taxus Element as the comparator (to
balloon was successful—ie, if an acceptable angiographic ensure that devices with similar agents were used), but
result was obtained (no higher-grade dissections National later (between June 19, 2013, and Jan 24, 2014) had to be
Heart, Lung, and Blood Institute grade C to F,18 no continued with Xience because the initial stent became
decreased blood flow (thrombolysis in myocardial unavailable.17 The sample size was increased to conform
infarction score ≤2), or no residual stenosis >30%) to the different efficacy of the two DES. PCI was done
according to consensus group rec ommendations.10 strictly in accordance with established guidelines.10
Exclusion criteria were concomitant PCI of large lesions Specifically, the DCB, which had to be 2–3 mm longer on
of at least 3 mm in diameter in the same epicardial each side than the predilatation balloon, was inflated at
coronary artery, PCI of in-stent restenosis, life expectancy nominal pressure for a minimal time of 30 s. In cases
of less than 12 months, pregnancy, enrolment in another with flow-limiting dissections or residual angiographically
randomised trial for coronary intervention, or inability to significant stenosis (ie, >30% stenosis) after DCB
give informed consent. All patients gave written informed treatment, additional spot stenting avoiding geographical
consent before the intervention started. In urgent cases mismatch was allowed. PCI was done under dual
when the intervention could not be postponed, oral antiplatelet therapy with acetylsalicylic acid (100 mg per
consent was given before the intervention started. Oral day) and either a thienopyridine (clopidogrel [75 mg per
consent was documented by a second medical person not day] or prasugrel [10 mg per day]) or ticagrelor (90 mg
involved in the trial; written informed consent was given twice per day). After PCI, dual antiplatelet therapy was
after the intervention. continued in stable patients for 4 weeks (for DCB) or
2 www.thelancet.com Published online August 28, 2018 http://dx.doi.org/10.1016/S0140-6736(18)31719-7
Articles
6 months (for DES) and in patients with acute coronary ZCU method to calculate the p value for non-inferiority.26
syndrome for 12 months.19 Dual antiplatelet therapy was For sensitivity analyses, we repeated non-inferiority
given for 3 months in patients treated with a comb analyses on the full analysis population.
ination of DCB and BMS, and for 6 months in patients The full-analysis population was defined as all patients
with DCB and DES. In patients on oral anticoagulation, matching inclusion criteria who provided informed
we followed the guidelines,1 irrespective of DCB or DES consent and were assigned to a treatment group. To form
treatment. the per-protocol population, we excluded patients from
All endpoints were adjudicated by an independent the full-analysis population with major protocol violations
critical events committee. Follow-up was done after 6 and (received neither DCB nor DES despite being randomised,
12 months with structured clinical questionnaires or unapproved procedures, received the opposite treatment
phone calls to assess clinical events, medication, and than randomised due to complications) or patients lost to
quality of life. follow-up. Patients in the per-protocol population were
analysed as treated. We used Cox proportional hazards
Outcomes models and Kaplan-Meier curves to analyse the time-
The primary objective of this trial was to show non- dependent occurrence of events; hazard ratios (HRs) are
inferiority of DCB versus DES regarding MACE after presented with 95% CI. For baseline characteristics,
12 months. MACE was defined as the composite of continuous variables are reported as mean and SD,
cardiac death, non-fatal myocardial infarction, and target whereas categorical variables are reported as frequency
vessel revascularisation. Cardiac death was defined as any and proportion. 95% CIs presented for secondary
death that was not clearly of extracardiac origin, and endpoints are not adjusted for multiple testing and
myocardial infarction, according to guidelines.20 Second inferences drawn from these might be not reproducible.
ary endpoints were the single components of the primary The primary analysis in the per-protocol population had
endpoint, probable or definite stent thrombosis according no missing values by definition. In sensitivity analyses
to the Academic Research Consortium definition,21 major on the full-analysis population, we assumed no event
bleeding (defined as Bleeding Academic Research for patients who were lost to follow-up. We analysed
Consortium type 3 to 5 bleeding),22 and net clinical benefit secondary endpoints in the full-analysis population,
(defined as the composite of MACE and major bleeding). according to the intention-to-treat principle with patients
Statistical analysis
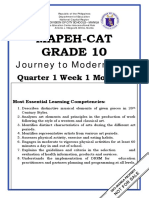
883 patients with percutaneous coronary
The required sample size to show non-inferiority of DCB intervention assessed for eligibility
versus DES in the primary endpoint at 12 months was
estimated to be 758 patients (appendix). This estimation
Predilatation
was done after the comparator stents were changed
(between June 19, 2013, and Jan 24, 2014) and was
calculated on the basis of an expected MACE rate
of 7% for DCB14 and 10% for DES,23 with non-inferiority Successful Flow-limiting dissection (TIMI
established if the upper limit of the two-sided 95% CI% score ≤2) or residual stenosis above
30% during predilatation
of the absolute risk difference was less than 4% (non-
inferiority margin). Because the event rates of paclitaxel-
eluting stents were expected to be higher than the rates 758 randomly allocated to treatment 125 assessed in separate registry
and included in full analysis set
of everolimus-eluting stents,24 we calculated the sample
size on the basis of the DES with expected lower event
rates. Sample size was calculated with a resampling
procedure (ie, we evaluated samples by sampling various 382 assigned to receive DCB 376 assigned to receive DES
sample sizes 9999 times from binomial distributions
based on expected rates) and was set to ensure at least
9 lost to follow-up or 13 lost to follow-up or
90% power (1–β=0·9) at a significance level of α=5%. To withdrawal of consent withdrawal of consent
account for an overall dropout rate of 5%, 758 patients 1 protocol violation 1 bare metal stent only
were needed to ensure 720 analysable patients. After the 2 treatment change due 1 protocol violation
to complication 2 treatment change due
enrolment of 75% of patients, a blinded re-assessment of to complication
sample size was done, which showed that the trial could
be continued without an increase in sample size.25 To test
370 followed up at 359 followed up at
for non-inferiority, the absolute difference in MACE risk 12 months and included 12 months and included
at 12 months between the DCB and DES groups and the in per-protocol set in per-protocol set
two-sided 95% CI was analysed in the per-protocol
population by applying a continuity corrected mod Figure 1: Trial profile
ification of Wilson’s score method. We used the TIMI=thrombolysis in myocardial infarction. DCB=drug-coated balloons. DES=drug-eluting stents.
www.thelancet.com Published online August 28, 2018 http://dx.doi.org/10.1016/S0140-6736(18)31719-7 3
Articles
Drug-coated Drug-eluting Drug-coated Drug-eluting
balloon (n=382) stent (n=376) balloon stent
Mean age, years 67·2 (10·3) 68·4 (10·3) Target vessel
Sex Left anterior descending artery 128 (34%) 116 (31%)
Male 295 (77%) 262 (70%) Left circumflex artery 179 (47%) 183 (49%)
Female 87 (23%) 114 (30%) Right coronary artery 75 (20%) 77 (20%)
Mean body-mass index 28·4 (4·5) 28·2 (4·6) Multivessel disease 313 (82%) 285 (76%)
Smoking status* Bifurcation lesion 22 (6%) 29 (8%)
Current smoker 82 (22%) 72 (20%) Mean procedural success, n (SD) 96% (19) 98 (13)
Former smoker 144 (39%) 123 (34%) Mean number of DCB or DES, n (SD) 1·68 (0·82) 1·26 (0·55)
No smoker 148 (40%) 172 (47%) Mean length of DCB or DES, mm (SD) 23·93 (11·74) 23·18 (12·85)
Hypercholesterolaemia† 262 (69%) 259 (70%) Mean effective size of DCB or 2·75 (2.14) 2·57 (0.25)
DES, mm (SD)
Arterial hypertension‡ 324 (85%) 332 (89%)
Mean inflation pressure, atm (SD) 11·06 (3·54) 13·58 (3·90)
Family history of CAD 150 (43%) 128 (38%)
Mean duration of inflation, sec (SD) 48·45 (28.24) 23·36 (18.92)
Diabetes§
Compliant balloon for predilatation 282 (73%) 276 (74%)
Insulin dependent 48 (13%) 47 (13%)
Data are n (%) or mean (SD). DCB=drug-coated balloons. DES=drug-eluting stents.
Non-insulin dependent 74 (19%) 83 (22%)
No diabetes 259 (68%) 243 (65%) Table 2: Angiographic data
Previous myocardial infarction 160 (42%) 133 (35%)
Previous PCI 235 (62%) 241 (64%)
Previous CABG 37 (10%) 34 (9%) data. The corresponding author had final responsibility
Cerebrovascular insult¶ for the decision to submit for publication.
No 352 (92%) 339 (90%)
Stroke 16 (4%) 23 (6%) Results
Transient ischaemic attack 13 (3%) 14 (4%) Between April 10, 2012, and February 1, 2017, 883 patients
PAOD 27 (7%) 26 (7%) were enrolled, of which 758 (86%) were randomly
COPD 28 (7%) 36 (9%) assigned to treatment and 125 (14%) entered a separate
Renal failure 54 (14%) 59 (16%) registry. Randomisation ended once the calculated
Presentation sample size was reached. Of the patients who were
STEMI 11 (3%) 4 (1%) randomly assigned treatment, 382 were assigned to the
NSTEMI 53 (14%) 56 (15%) DCB group and 376 to the DES group. Overall, 729 (96%)
Unstable angina 48 (13%) 42 (11%) of 758 patients had complete data for the primary
Stable angina 270 (70%) 274 (73%) endpoint (figure 1). The two treatment groups were well
Oral anticoagulation 33 (9%) 31 (8%) balanced in terms of baseline demographic and clinical
LVEF, median (IQR) 60% (50–60) 60% (55–65) characteristics of patients (table 1) and angiographic data
(table 2). However, there was a higher proportion of men
Data are n (%) or mean (SD) unless otherwise stated. CAD=coronary artery
disease. PCI=percutaneous coronary intervention. CABG=coronary artery bypass
in the DCB group than in the DES group (p=0·0232;
graft. PAOD=peripheral arterial occlusive disease. COPD=chronic obstructive table 1).
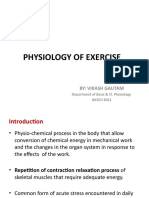
pulmonary disease. STEMI=ST-elevation myocardial infarction. The difference in absolute risk of MACE between the
NSTEMI=non-ST-elevation myocardial infarction. LVEF=left ventricular ejection
two treatment groups was 0·0005 (95% CI –0·038 to 0·039)
fraction. *Data were only available for 374 participants in the drug-coated balloon
group and 367 in the drug-eluting stent group. †Data were only available for in the per-protocol population (figure 2). Since the margin
381 in the drug-coated balloon group and 370 in the drug-eluting stent group. of the 95% CI did not cross the predefined value of 4%
‡Data were only available for 374 in the drug-eluting stent group. §Data were only (p=0·0217), non-inferiority of DCB versus DES was shown
available for 381 in the drug-coated balloon group and 373 in the drug-eluting
stent group. ¶Data were only available for 381 in the drug-coated balloon group. (figure 2). A sensitivity analysis in the full-analysis
population gave similar results, with a difference in risk of
Table 1: Baseline characteristics
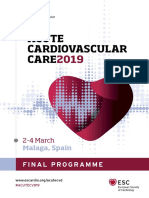
–0·0012 (–0·040 to 0·037; figure 2). In the full-analysis
population, proportion of MACE events after 12 months
analysed as randomised. We used R (version 3.5.0) for all was 7·3% in the DCB group and 7·5% in the DES group
statistical analyses.27 (0·97, 0·58–1·64; p=0·9180; figure 3).
Rates of cardiac death (12 patients [3·1%] for the DCB
Role of the funding source group vs five patients [1·3%] for the DES group; HR 2·33
The funders of the study had no role in study design, [95% CI 0·82–6·61]; p=0·1131), non-fatal myocardial
data collection, data analysis, and data interpretation, or infarction (1·6% vs 3·5%; 0·46 [0·17–1·20]; p=0·1123),
writing of the report, and did not participate in the and target vessel revascularisation (3·4% vs 4·5%; 0·75
decision to submit the manuscript for publication. The [0·36–1·55]; p=0·4375) did not differ between the groups
principle investigator (RVJ) and NG had full access to all (appendix). Probable or definite stent thrombosis occurred
4 www.thelancet.com Published online August 28, 2018 http://dx.doi.org/10.1016/S0140-6736(18)31719-7
Articles
in both treatment groups since stents were also implanted
Events, n/N (%) DCB (%) - DES (%) Difference (95% CI) p value
in patients in the DCB group, mostly in other parts of the
coronary vasculature; however, rates were low and not Per-protocol population
statistically different between the DCB and DES groups DES 27/359 (8%)
DCB 28/370 (8%) 0·0005 (−0.038 to 0.039) 0·0217
(0·79% vs 1·60%; 0·73 [0·16–3·26]). There was no acute
Full analysis population
vessel closure in DCB lesions. Rates of major bleeding
DES 28/376 (7%)
were low and similar between the DCB and DES groups
DCB 28/382 (7%) –0·0012 (−0.040 to 0.037) 0·0152
(1·1% vs 2·4%; 0·45 [0·14–1·46]) and rates of the net
clinical benefit were similar in the DCB and DES groups –0·06 –0·04 –0·02 0 0·02 0·04 0·06
(7·9% vs 9·6%; 0·81 [0·50–1·32]). None of the subgroups Favours DCB Favours DES
showed strong differential effects between the treatment
Figure 2: Major adverse cardiac events by study group
groups (interaction tests; figure 4). Data are absolute difference in event rates between the DCB and DES groups. The p-value tests whether the
MACE proportions after 12 months were generally absolute difference in rates is equal to the pre-defined non-inferiority margin (0·04). DCB=drug-coated balloons.
higher in men than in women but were similar within DES=drug-eluting stents.
both treatment groups (figure 4). The interaction did not
differ between sex and treatment (interaction term 0·93
0·20 DES
[0·25–3·41]; p=0·9127). DCB
Within the two treatment groups, we did specific post-
hoc analyses regarding the combination of DCB with stents
0·15
(DCB group) and the different stent types (DES group; per-
Cumulative MACE event rate
protocol population; figure 5). In the DCB group, 19 (5·1%)
patients were treated with a combination of DCB and
stents in the index lesion (mostly DES). MACE rates for 0·10
DCB and stents were numerically higher than for DCB
only (DCB with stent vs DCB only, 15·8% vs 7·0%; HR 2·11
[95% CI 0·62–7·19]; p=0·2306). In the DES group, 94 0·05
(28%) of 341 patients were treated with paclitaxel-eluting
stents, which had numerically higher MACE rates than did
everolimus-eluting stents (12·8% vs 5·7%, HR 2·04 0
[0·88–4·76]; p=0·0987). The specific HR for the comparison 0 30 60 90 120 150 180 210 240 270 300 330 360
Follow-up (days)
between DCB and everolimus-eluting stents was 1·21 Number at risk
(0·63–2·32; p=0·5751) and was 0·52 (0·26 to 1·04; DES 376 366 360 355 355 350 346 337 333 332 331 317 284
DCB 382 376 373 371 368 367 362 351 347 346 343 326 295
p=0·0649) for the comparison between DCB and paclitaxel-
eluting stents. Figure 3: Cumulative incidence rates for MACE
Full analysis population. MACE=major adverse cardiac events. DCB=drug-coated balloons. DES=drug-eluting
Discussion stents.
The BASKET-SMALL 2 trial showed the non-inferiority
of DCB versus DES regarding clinical events in a large plain balloon angioplasty—at that time in the absence
all-comer population undergoing PCI in native small- of dual antiplatelet therapy—was restricted by acute
vessel coronary artery disease. After 12 months, MACE vessel closure due to elastic recoil and flow-limiting
rates were low and similar between the groups. dissections.28 Therefore, in our study, rigorous lesion
The DCB technique is based on the interaction of a preparation according to established recommendations10
highly lipophilic drug with a coating matrix and allows to achieve an acceptable angiographic result before use
for fast and homogenous drug delivery into the vessel of DCB was mandatory to avoid complications.
wall. Although many devices exist on the market, So far, only two randomised controlled trials have
balloons coated with paclitaxel and iopromide have assessed the efficacy and safety of DCB versus DES in
shown favourable clinical results and are the most native small-vessel coronary artery disease.15,16 The
widely used to date.9 DCB is an established treatment PICCOLETO study15 tested the effect of a paclitaxel-
option for the treatment of in-stent restenosis,5–8 but, eluting balloon (Dior; Eurocor, Bonn, Germany), in
in native small-vessel coronary artery disease, the which the drug adhered to the roughened surface without
technique has been tested in smaller studies only.15,16 matrix, compared with a first-generation paclitaxel-
Advantages of DCB are the potential for favourable eluting stent (Taxus Liberté) and was prematurely
vascular remodelling after angioplasty in the absence of stopped after 57 patients were enrolled. The findings
a stent, the theoretical lack of any stent thrombosis, and showed an increase in the primary angiographic
the option of shortening dual antiplatelet therapy to endpoint (% diameter stenosis) in the DCB group versus
only 4 weeks. Possible limitations relate to the early days the DES group after 6 months and also an increase in the
of interventional cardiology, in which the method of combined clinical endpoint, which was mainly attributed
www.thelancet.com Published online August 28, 2018 http://dx.doi.org/10.1016/S0140-6736(18)31719-7 5
Articles
MACE, n/N (%) Hazard ratio (95% CI) pinteraction
DCB DES
Age, years 0·3595
<75 17/278 (6%) 20/256 (8%) 0·93 (0·79–1·10)
≥75 11/104 (11%) 8/120 (7%) 1·06 (0·81–1·39)
Sex 0·9127
Female 5/87 (6%) 7/114 (6%) 1·21 (0·37–4·01)
Male 23/295 (8%) 21/262 (8%) 0·93 (0·52–1·69)
Renal disease 0·9577
Yes 9/91 (10%) 8/83 (10%) 0·99 (0·38–2·57)
No 19/291 (7%) 20/293 (7%) 0·95 (0·50–1·78)
ACS 0·0856
Yes 7/112 (6%) 12/102 (12%) 0·49 (0·19–1·25)
No 21/270 (8%) 16/274 (6%) 1·29 (0·67–2·47)
Diabetes 0·3017
Yes 12/122 (10%) 16/130 (12%) 0·83 (0·38–1·81)
No 16/260 (6%) 12/246 (5%) 1·37 (0·64–2·90)
Multivessel disease 0·3982
Yes 26/313 (8%) 23/285 (8%) 1·03 (0·59–1·82)
No 2/69 (3%) 5/91 (5%) 0·45 (0·09–2·34)
Long lesion 0·5020
Yes 10/97 (10%) 4/59 (7%) 1·32 (0·40–4·32)
No 18/284 (6%) 24/317 (8%) 0·86 (0·46–1·58)
Bifurcation 0·4501
Yes 2/22 (9%) 5/29 (17%) 0·45 (0·08–2·39)
No 26/356 (7%) 22/333 (7%) 1·11 (0·63–1·95)
0·12 0·25 0·50 1·0 2·0 4·0
Favours DCB Favours DES
Figure 4: Subgroup analyses of MACE and hazard ratios
Cox proportional hazards models were fitted with time-to-MACE as outcome and with patients censored at last observation if experiencing no event. All analyses
were done on the full analysis population with the treatment group as assigned to patients at randomisation. MACE=major adverse cardiac events. DCB=drug-coated
balloons. DES=drug-eluting stents. ACS=acute coronary syndrome.
0·20 DCB
to the type of DCB and the fact that geographical
DCB+DES mismatch was not prevented.29 By contrast, the BELLO
Taxus study16 tested the efficacy of a paclitaxel-eluting balloon
Xience
using urea as matrix (IN.PACT Falcon; Medtronic, Santa
0·15
Rosa, CA, USA) against a first-generation paclitaxel-
Cumulative MACE event rate
eluting stent (Taxus Liberté) and enrolled 182 patients.
The primary angiographic endpoint of non-inferiority
0·10 regarding angiographic in-stent or in-balloon late loss
after 6 months was met, and the combined clinical
endpoint showed similar event rates for both groups
0·05 after 6 and 36 months.30 Although more than 95% of
lesions were treated with optimal lesion preparation in
BELLO, this measurement was true for only 25% of
0 lesions in PICCOLETO. Therefore, the use of a DCB
0 30 60 90 120 150 180 210 240 270 300 330 360
with favourable clinical data, the prevention of geo
Follow up (days)
Number at risk graphical mismatch and an optimal lesion preparation
DCB 356 352 349 348 346 345 340 335 332 331 328 311 284
DCB+DES 19 19 19 18 18 18 18 17 17 17 17 17 13
might have contributed to the positive result of BASKET-
Taxus 93 90 88 87 87 86 85 82 81 81 81 80 80 SMALL 2. The study was not powered to detect dif
Xience 243 239 236 233 233 229 229 228 227 226 225 212 185 ferences in the single components of the primary
endpoint. The potential long-term benefit of DCB over
Figure 5: Cumulative incidence rates for MACE
According to the actual treatment that patients received. MACE=major adverse cardiac events. permanently implanted stents might not be seen until
DCB=drug-coated balloons. DES=drug-eluting stents. after 2–5 years.30 Long-term follow-up data of the current
study are still being collected and will be reported in
due time.
6 www.thelancet.com Published online August 28, 2018 http://dx.doi.org/10.1016/S0140-6736(18)31719-7
Articles
Two distinct interventional treatment entities in our trial small native coronary artery disease might safely be
are of specific interest. The numerically (not significantly) treated with DCB after successful predilatation.
higher event rate with the combination of DCB and stents Contributors
might be explained by accidental angiographic mismatch RVJ, NG, CK, and BS designed the study, collected and interpreted the
and is consistent with previous data, wherein rates of data, and drafted the manuscript. AF, M-AO, NM, SM-W, GL, DW, JW,
SR, MS, FM, AL, F-PS, CM, PR, and SO collected the data and
restenosis increased when DCB were combined with critically revised the work for important intellectual content.
BMS.14,15 Therefore, guidelines on DCB therapy advocate MC designed the study and analysed the data. All authors approved
the use of DES in case of unplanned stent implantation,10 the final version.
and current generation limus-DES should be preferred.31 Declaration of Interests
However, the combination of DCB with stents in the same RVJ has received lecture honoraria and travel support from B Braun.
lesion should be avoided whenever possible. Second, the M-AO has received proctoring honoraria and travel support from
Biosensors and research support from Terumo. NM has received
MACE rates of patients on DES who are receiving speaker’s honoraria from Edwards and Medtronic and consultant
paclitaxel-eluting stents compared with that of patients honoraria from Biotronik. GL is a medical user advisory board member
receiving everolimus-eluting stents is consistent with for REVA Medical and has relationships with drug and device companies,
previous non-randomised data.23,24 However, a randomised including Terumo, Acrostak, Bionsensors, Boston Scientific, Abbott
Vascular, Impuls Medical, and Orbus Neich. FM is supported by Deutsche
controlled pilot study in small-vessel coronary artery Gesellschaft für Kardiologie, Deutsche Hochdruckliga, and Deutsche
disease reported a numerically lower event rate for Forschungsgemeinschaft (SFB TRR 219), and has received grant support
paclitaxel-eluting versus zotarolimus-eluting stents.32 On and personal fees from Medtronic and Recor Medical. AL has received
the basis of our data, paclitaxel seems to be more efficient speaker honoraria or served as a consultant for the following companies:
Medtronic, St Jude Medical, Claret Medical Inc, Boston Scientific,
in the setting of the DCB than the DES technique. Edwards Lifesciences, Symetis, and Bard, and holds stock options from
DCB require a shorter dual antiplatelet therapy than do Claret Medical, Emboline, and Transverse Medical. AL has also received
DES in stable patients (ie, 4 weeks only instead of grant support from Medtronic and Claret Medical and speaker honoraria
from Novartis and Bayer. NG has received travel support from B Braun.
6 months), which might reduce the risk of major
BS is a shareholder of InnoRa GmbH and was named as co-inventor on
bleeding.10,19 The shorter duration of dual antiplatelet patent applications submitted by Charité University Hospital, Berlin,
therapy might be of additional benefit, which was not Germany. All other authors declare no competing interests.
accounted for in the current non-inferiority trial. Data sharing
Our study has some limitations. First, the trial was As secondary analyses are in progress, data collected for the study,
initially designed with a second-generation paclitaxel- including individual participant data and a data dictionary defining each
field in the set, will not be made available to others.
eluting stent as comparator to the paclitaxel-eluting
balloon to use the same drug and make comparisons Acknowledgments
The study was supported by Schweizerischer Nationalfonds zur Förderung
possible. However, since the stent became unavailable der Wissenschaftlichen Forschung (32003B_140956), Basel Cardiovascular
during the study, the comparator was changed to an Research Foundation, and B Braun Medical AG, Switzerland.
everolimus-eluting stent and the sample size was References
increased. Therefore, the trial was switched from a pure 1 Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS Guidelines
comparison of two different devices to a more compre on myocardial revascularization: The Task Force on Myocardial
Revascularization of the European Society of Cardiology (ESC) and
hensive comparison of two interventional strategies. the European Association for Cardio-Thoracic Surgery (EACTS)
Second, there was an imbalance in sex distribution developed with the special contribution of the European Association
among the randomised groups, with more male patients of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J
2014; 35: 2541–619.
randomly assigned to the DCB group than to the DES 2 Schunkert H, Harrell L, Palacios IF. Implications of small reference
group. However, a specific analysis revealed that male vessel diameter in patients undergoing percutaneous coronary
patients had higher event rates than women did, thus revascularization. J Am Coll Cardiol 1999; 34: 40–48.
3 Moreno R, Fernández C, Alfonso F, et al. Coronary stenting versus
underlining the efficacy of DCB and that there was no balloon angioplasty in small vessels: a meta-analysis from
significant interaction between sex and treatment. Third, 11 randomized studies. J Am Coll Cardiol 2004; 43: 1964–72.
extrapolation of our findings to other types of DCB may 4 Siontis GC, Piccolo R, Praz F, et al. Percutaneous coronary
interventions for the treatment of stenoses in small coronary arteries:
not be justified. Finally, there was no routine angiographic a network meta-analysis. JACC Cardiovasc Interv 2016; 9: 1324–34.
follow-up in the study; therefore, event rates could have 5 Scheller B, Hehrlein C, Bocksch W, et al. Treatment of coronary
been underestimated. Since this was a clinical trial, there in-stent restenosis with a paclitaxel-coated balloon catheter.
was no routine core-lab analysis of the angiographies at N Engl J Med 2006; 355: 2113–24.
6 Unverdorben M, Vallbracht C, Cremers B, et al. Paclitaxel-coated
trial entry and at follow-up. balloon catheter versus paclitaxel-coated stent for the treatment of
In summary, to our knowledge, BASKET-SMALL 2 is coronary in-stent restenosis. Circulation 2009; 119: 2986–94.
the first large randomised controlled trial testing the 7 Rittger H, Brachmann J, Sinha AM, et al. A randomized, multicenter,
single-blinded trial comparing paclitaxel-coated balloon angioplasty
efficacy of a paclitaxel-iopromide-coated DCB versus with plain balloon angioplasty in drug-eluting stent restenosis:
second-generation DES in a large all-comer population the PEPCAD-DES study. J Am Coll Cardiol 2012; 59: 1377–82.
regarding clinical endpoints. Our study showed that 8 Byrne RA, Neumann FJ, Mehilli J, et al. Paclitaxel-eluting balloons,
paclitaxel-eluting stents, and balloon angioplasty in patients with
DCB are non-inferior to DES in lesions of small native restenosis after implantation of a drug-eluting stent
coronary arteries regarding MACE up to 12 months, with (ISAR-DESIRE 3): a randomised, open-label trial. Lancet 2013;
similar event rates for both treatment groups. Therefore, 381: 461–67.
www.thelancet.com Published online August 28, 2018 http://dx.doi.org/10.1016/S0140-6736(18)31719-7 7
Articles
9 Alfonso F, Scheller B. State of the art: balloon catheter 21 Cutlip D, Windecker S, Mehran R, et al. Clinical end points in
technologies–drug-coated balloon. EuroIntervention 2017; coronary stent trials: a case for standardized definitions. Circulation
13: 680–95. 2007; 115: 2344–51.
10 Kleber FX, Rittger H, Bonaventura K, et al. Drug-coated balloons 22 Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding
for treatment of coronary artery disease: updated recommendations definitions for cardiovascular clinical trials: a consensus report
from a consensus group. Clin Res Cardiol 2013; 102: 785–97. from the Bleeding Academic Research Consortium. Circulation
11 Venetsanos D, Lawesson SS, Panayi G, et al. Long-term efficacy of 2011; 123: 2736–47.
drug coated balloons compared with new generation drug-eluting 23 Cannon LA, Simon DI, Kereiakes D, et al. The XIENCE nano
stents for the treatment of de novo coronary artery lesions. everolimus eluting coronary stent system for the treatment of small
Catheter Cardiovasc Interv 2018; published online Feb 26. coronary arteries: the SPIRIT Small Vessel trial.
DOI:10.1002/ccd.27548. Catheter Cardiovasc Interv 2012; 80: 546–53.
12 Waksman R, Serra A, Loh JP, et al. Drug-coated balloons for de 24 Cannon LA, Kereiakes DJ, Mann T, et al. A prospective evaluation of
novo coronary lesions: results from the Valentines II trial. the safety and efficacy of TAXUS Element paclitaxel-eluting
EuroIntervention 2013; 9: 613–19. coronary stent implantation for the treatment of de novo coronary
13 Vaquerizo B, Miranda-Guardiola F, Fernández E, et al. Treatment of artery lesions in small vessels: the PERSEUS Small Vessel trial.
small vessel disease with the paclitaxel drug-eluting balloon: EuroIntervention 2011; 6: 920–27.
6-month angiographic and 1-year clinical outcomes of the Spanish 25 Friede T, Mitchell C, Müller-Velten G. Blinded sample size
Multicenter Registry. J Interv Cardiol 2015; 28: 430–38. reestimation in non-inferiority trials with binary endpoints.
14 Unverdorben M, Kleber F, Heuer H, et al. Treatment of small Biom J 2007; 49: 903–16.
coronary arteries with a paclitaxel-coated balloon catheter. 26 Kawasaki Y, Zhang F, Miyaoka E. Comparisons of test statistics for
Clin Res Cardiol 2010; 99: 165–74. non-inferiority test for the difference between two independent
15 Cortese B, Micheli A, Picchi A, et al. Paclitaxel-coated balloon versus binomial proportions. Am J Biostat 2010; 1: 23–31.
drug-eluting stent during PCI of small coronary vessels, 27 R Core Team. R: A language and environment for statistical
a prospective randomised clinical trial. The PICCOLETO study. computing. Vienna, Austria: R Foundation for Statistical
Heart 2010; 96: 1291–96. Computing, 2018.
16 Latib A, Colombo A, Castriota F, et al. A randomized multicenter 28 Dorros G, Cowley MJ, Simpson J, et al. Percutaneous transluminal
study comparing a paclitaxel drug-eluting balloon with a coronary angioplasty: report of complications from the National
paclitaxel-eluting stent in small coronary vessels: the BELLO Heart, Lung, and Blood Institute PTCA Registry. Circulation 1983;
(Balloon Elution and Late Loss Optimization) study. 67: 723–30.
J Am Coll Cardiol 2012; 60: 2473–80. 29 Cortese B. The PICCOLETO study and beyond. EuroIntervention
17 Gilgen N, Farah A, Scheller B, et al. Drug-coated balloons for de 2011; 7: K53–56.
novo lesions in small coronary arteries: rationale and design of 30 Latib A, Ruparelia N, Menozzi A, et al. 3-year follow-up of the
BASKET-SMALL 2. Clin Cardiol 2018; 41: 569–75. Balloon Elution and Late Loss Optimization Study (BELLO).
18 Huber MS, Mooney JF, Madison J, Mooney MR. Use of a JACC Cardiovasc Interv 2015; 8: 1132–34.
morphologic classification to predict clinical outcome after 31 Mok KH, Wickramarachchi U, Watson T, Ho HH, Eccleshall S,
dissection from coronary angioplasty. Am J Cardiol 1991; 68: 467–71. Ong PJL. Safety of bailout stenting after paclitaxel-coated balloon
19 Valgimigli M, Bueno H, Byrne RA, et al. 2017 ESC focused update angioplasty. Herz 2017; 42: 684–89.
on dual antiplatelet therapy in coronary artery disease developed in 32 Jeger R, Pfisterer M, Pfister O, et al. First-generation
collaboration with EACTS: the task force for dual antiplatelet paclitaxel- vs. second-generation zotarolimus-eluting stents in small
therapy in coronary artery disease of the European Society of coronary arteries: the BASKET-SMALL pilot study.
Cardiology (ESC) and of the European Association for Postepy Kardiol Interwencyjnej 2016; 12: 314–20.
Cardio-Thoracic Surgery (EACTS). Eur Heart J 2018; 39: 213–60.
20 Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of
myocardial infarction. J Am Coll Cardiol 2012; 60: 1581–98.
8 www.thelancet.com Published online August 28, 2018 http://dx.doi.org/10.1016/S0140-6736(18)31719-7
You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Electric Alex 519171918 GernDocument950 pagesElectric Alex 519171918 GernShyamSoniNo ratings yet
- Comparative Anatomy of Heart, Circulation Aortic Arches EtcDocument36 pagesComparative Anatomy of Heart, Circulation Aortic Arches EtcNarasimha Murthy100% (4)
- Ipi Nursing Part 1,2,3Document53 pagesIpi Nursing Part 1,2,3Noleen MckayNo ratings yet
- Mapeh-Cat Grade 10: Journey To Modern Life!Document41 pagesMapeh-Cat Grade 10: Journey To Modern Life!SophiaRosalesTamidles67% (3)
- Novel Tools For Hemodynamic Monitoring in Critically Ill Patients With Shock - UpToDateDocument26 pagesNovel Tools For Hemodynamic Monitoring in Critically Ill Patients With Shock - UpToDateAlex KuliaNo ratings yet
- Bmj.l5101.full Stroke PDFDocument15 pagesBmj.l5101.full Stroke PDFMr. LNo ratings yet
- Transfusion Hemolytic PDFDocument13 pagesTransfusion Hemolytic PDFMr. LNo ratings yet
- Anticoagulante EP PDFDocument4 pagesAnticoagulante EP PDFMr. LNo ratings yet
- NEJM 2 5 Mack Tavi1Document11 pagesNEJM 2 5 Mack Tavi1Mr. LNo ratings yet
- Porta Lvenu Sgain (Immagine)Document1 pagePorta Lvenu Sgain (Immagine)Mr. LNo ratings yet
- Lancet Diabete PDFDocument11 pagesLancet Diabete PDFMr. LNo ratings yet
- 10 1056@NEJMra1706174Document12 pages10 1056@NEJMra1706174Mr. LNo ratings yet
- Lichen Planus: Images in Clinical MedicineDocument1 pageLichen Planus: Images in Clinical MedicineMr. LNo ratings yet
- Clinical Picture: Jia-Wei Liu, Dong-Lai MaDocument1 pageClinical Picture: Jia-Wei Liu, Dong-Lai MaMr. LNo ratings yet
- Semi Detailed Lesson PlanDocument31 pagesSemi Detailed Lesson PlanJonathan Tabbun100% (1)
- OLYMPUS Thunderbeat OEJ Manual 20141127Document64 pagesOLYMPUS Thunderbeat OEJ Manual 20141127Marcos ZanchetNo ratings yet
- Healthier - by Dr. RawatDocument112 pagesHealthier - by Dr. RawatritikaNo ratings yet
- Demo-Teaching DLP - MidayDocument10 pagesDemo-Teaching DLP - MidayCoLavs AvenueNo ratings yet
- Oxygen Insufficiency.Document54 pagesOxygen Insufficiency.Josephine George JojoNo ratings yet
- Dog Dissection ProcedureDocument20 pagesDog Dissection ProcedureChristine Joyce NavarroNo ratings yet
- Preload and AfterloadDocument28 pagesPreload and Afterloadapi-19916399100% (1)
- Referat EndocarditisDocument25 pagesReferat EndocarditisNadya Hasna Rasyida DANo ratings yet
- A P2 1Document36 pagesA P2 1Priya_Vankovic_7963No ratings yet
- Paida Lajin Self-Healing EnglishDocument69 pagesPaida Lajin Self-Healing EnglishKarma Arnab100% (2)
- Student Exploration: Circulatory SystemDocument4 pagesStudent Exploration: Circulatory SystemAndreNo ratings yet
- Heart Attack and EmphysemaDocument12 pagesHeart Attack and EmphysemaKylie Adrianna Bernabe SarmientoNo ratings yet
- Ventricular Septal Defects Embryology and Imaging.11Document7 pagesVentricular Septal Defects Embryology and Imaging.11Esra SiddigNo ratings yet
- Acute/Critically Ill Patients in Hemodynamic Monitoring (Assessment)Document6 pagesAcute/Critically Ill Patients in Hemodynamic Monitoring (Assessment)Esmareldah Henry SirueNo ratings yet
- Endodontics in Systemically Compromised PatientsDocument30 pagesEndodontics in Systemically Compromised Patientscarolina pavezNo ratings yet
- The Anatomy of The Coronary SinusDocument7 pagesThe Anatomy of The Coronary Sinusmihalcea alinNo ratings yet
- Chronic Total OcclusionsDocument37 pagesChronic Total OcclusionsValentin CHIONCELNo ratings yet
- Insuficienta Venoasa CronicaDocument15 pagesInsuficienta Venoasa CronicaSimona IonitaNo ratings yet
- Circulatory System FKM'12Document55 pagesCirculatory System FKM'12muhammadsudrajadNo ratings yet
- Anjleena: Curriculum VitaeDocument2 pagesAnjleena: Curriculum Vitaetonny buddyNo ratings yet
- Big Data Analytics in Heart Attack Prediction 2167 1168 1000393Document9 pagesBig Data Analytics in Heart Attack Prediction 2167 1168 1000393jagadeeswara71No ratings yet
- Physiology of Exercise: By: Vikash GautamDocument27 pagesPhysiology of Exercise: By: Vikash GautamdevdsantoshNo ratings yet
- Arjun (Terminalia Arjuna) : MonographDocument3 pagesArjun (Terminalia Arjuna) : MonographSweta SrivastavaNo ratings yet
- 66Document84 pages66Jimmy Jimmy0% (1)
- Lesson 1.2 - Circulatory and Respiratory SystemsDocument24 pagesLesson 1.2 - Circulatory and Respiratory SystemsNabeel ShahidNo ratings yet