You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Symptom Conductive Hearing Loss.3Document3 pagesSymptom Conductive Hearing Loss.3Muhammad Pringgo ArifiantoNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Perioperative Antibiotic Prophylaxis in Open Tracheostomy A PreliminaryDocument6 pagesPerioperative Antibiotic Prophylaxis in Open Tracheostomy A PreliminaryMuhammad Pringgo ArifiantoNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
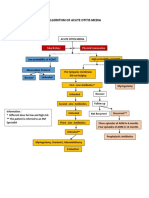
- Algorithm Acute Otitis MediaDocument1 pageAlgorithm Acute Otitis MediaMuhammad Pringgo ArifiantoNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Thyroid NoduleDocument7 pagesThyroid NodulePradhana FwNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Management of Esophageal Foreign Bodies - A Report On 26 Patients and Literature Review (#72399) - 62028Document5 pagesManagement of Esophageal Foreign Bodies - A Report On 26 Patients and Literature Review (#72399) - 62028Muhammad Pringgo ArifiantoNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Anterior Cruciate Ligament Injuries in The Skeletally Immature (Pringgo)Document12 pagesAnterior Cruciate Ligament Injuries in The Skeletally Immature (Pringgo)Muhammad Pringgo ArifiantoNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Acute Otitis Media Diagnosis and Treatment AlgorithmDocument1 pageAcute Otitis Media Diagnosis and Treatment AlgorithmMuhammad Pringgo ArifiantoNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Acute Otitis Media Diagnosis and Treatment AlgorithmDocument1 pageAcute Otitis Media Diagnosis and Treatment AlgorithmMuhammad Pringgo ArifiantoNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- System Policy Manual: Facility NameDocument14 pagesSystem Policy Manual: Facility NameMuhammad Pringgo ArifiantoNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Problem Hypotesis Mechanism More Info Learning Issue Problem SolvingDocument2 pagesProblem Hypotesis Mechanism More Info Learning Issue Problem SolvingMuhammad Pringgo ArifiantoNo ratings yet
- Ogexamination 110401040414 Phpapp02 PDFDocument26 pagesOgexamination 110401040414 Phpapp02 PDFDika RizkiardiNo ratings yet
- Acute Traumatic Posterior Shoulder Dislocation PDFDocument8 pagesAcute Traumatic Posterior Shoulder Dislocation PDFMuhammad Pringgo ArifiantoNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- JURNALDocument12 pagesJURNALAsMiraaaaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Fetal MonitoringDocument22 pagesFetal MonitoringMuhammad Pringgo ArifiantoNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Fetal MonitoringDocument22 pagesFetal MonitoringMuhammad Pringgo ArifiantoNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 13.revised Rate ListDocument51 pages13.revised Rate ListAsif Icbal100% (1)
- Pathophysiology Q's 1Document68 pagesPathophysiology Q's 1alibel_belloNo ratings yet
- Jama Sharma 2022 RV 220013 1660585212.14221Document9 pagesJama Sharma 2022 RV 220013 1660585212.14221Jatin YegurlaNo ratings yet
- National Medical Examination Review - PathologyDocument61 pagesNational Medical Examination Review - PathologyAnonymous ZUQcbcNo ratings yet
- Doc-Gerd Infographic Final PDFDocument1 pageDoc-Gerd Infographic Final PDFIndhumathiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 500 Nuggets CK CourseDocument36 pages500 Nuggets CK Coursepangea80No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Guidelines For Surgical Treatment of Gastroesophageal Reflux Disease GERDDocument48 pagesGuidelines For Surgical Treatment of Gastroesophageal Reflux Disease GERDMateo TamayoNo ratings yet
- Study Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesDocument10 pagesStudy Guide 1 Assessment of Digestive and Gastrointestinal Function and Treatment ModalitiesKc Cabanilla LizardoNo ratings yet
- Case Study No.4 The Telltale Heart: Group 2 Nuñez, Refuerzo, Abalos, Almonte, AlmueteDocument11 pagesCase Study No.4 The Telltale Heart: Group 2 Nuñez, Refuerzo, Abalos, Almonte, AlmueteRejeanne MonroyNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Clincher Notes for Rheumatology, Hematology, Infectious Diseases, Respiratory, Cardiovascular and NeurologyDocument22 pagesClincher Notes for Rheumatology, Hematology, Infectious Diseases, Respiratory, Cardiovascular and NeurologyvarrakeshNo ratings yet
- Atlas of Minimally Invasive Surgery in Esophageal Carcinoma (Puntambekar)Document203 pagesAtlas of Minimally Invasive Surgery in Esophageal Carcinoma (Puntambekar)Ciprian-Nicolae MunteanNo ratings yet
- Esophageal Atresia: Elvita Rahmi DaulayDocument21 pagesEsophageal Atresia: Elvita Rahmi DaulayabdullahshiddiqadamNo ratings yet
- Mammalian System-01 (Digestive System)Document35 pagesMammalian System-01 (Digestive System)Saumya99No ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Colon Cancer Risk Factors and Precancerous LesionsDocument14 pagesColon Cancer Risk Factors and Precancerous LesionsEssam ZayedNo ratings yet
- Diseases of OesophagusDocument46 pagesDiseases of OesophagusBrother GeorgeNo ratings yet
- Gastric CancerDocument7 pagesGastric CancerMicah PingawanNo ratings yet
- MCQs Mock Exams for General Surgery Board ExamDocument5 pagesMCQs Mock Exams for General Surgery Board ExamMoiz AhmedNo ratings yet
- Dysphagia Causes and DiagnosisDocument46 pagesDysphagia Causes and DiagnosisnanohaniwiekoNo ratings yet
- Feeding ArvedsonDocument10 pagesFeeding ArvedsonPablo Oyarzún Dubó100% (1)
- Dysphagia and Cervical Spine Disorders ReviewDocument12 pagesDysphagia and Cervical Spine Disorders Review박진영No ratings yet
- Hiatal HerniaDocument30 pagesHiatal HerniaAngelica Mercado SirotNo ratings yet
- Medical Terminology Express A Short Course Approach by Body System 2Nd Edition Gylys Test Bank Full Chapter PDFDocument34 pagesMedical Terminology Express A Short Course Approach by Body System 2Nd Edition Gylys Test Bank Full Chapter PDFDebraBurtonkfman100% (10)
- Taste buds highest in fungiform papillaeDocument19 pagesTaste buds highest in fungiform papillaePurple Ivy GuarraNo ratings yet
- Endoscopy, Barium MealDocument22 pagesEndoscopy, Barium Mealyudhisthir panthiNo ratings yet
- Republic of The Philippines Tamag, Vigan City 2700 Ilocos SurDocument23 pagesRepublic of The Philippines Tamag, Vigan City 2700 Ilocos SurJewel Ramos GalinatoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Digestive SystemDocument28 pagesDigestive Systemtessacruz1186No ratings yet
- A&P 2 - Digestive System Flashcards - QuizletDocument1 pageA&P 2 - Digestive System Flashcards - QuizletMunachande KanondoNo ratings yet
- Human body systems guideDocument26 pagesHuman body systems guideAntonio Fernando LimaNo ratings yet
- Int DX II Exam 2 Study Guide - Updated (Anon)Document5 pagesInt DX II Exam 2 Study Guide - Updated (Anon)bjpalmerNo ratings yet
- Case Reporrt GerdDocument7 pagesCase Reporrt GerdKarina WidyaNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)