You might also like
- PR Dr. AriadneDocument8 pagesPR Dr. AriadneSofia KusumadewiNo ratings yet
- Dabigatran in Primary SPAFDocument31 pagesDabigatran in Primary SPAFSofia KusumadewiNo ratings yet
- Arritmias SupraventricularesDocument62 pagesArritmias Supraventricularesapi-3826574No ratings yet
- Dabigatran in Primary SPAFDocument9 pagesDabigatran in Primary SPAFJessica StephanieNo ratings yet
- Visceral Paint of PeopleDocument6 pagesVisceral Paint of PeopleLiLies VathirahNo ratings yet
- Absensi PersonalDocument3 pagesAbsensi PersonalSofia KusumadewiNo ratings yet
- Role of Prostacyclin Analogue in The Management Patient With Pulmonary HypertensionDocument9 pagesRole of Prostacyclin Analogue in The Management Patient With Pulmonary HypertensionSofia KusumadewiNo ratings yet
- Thrombolysis Pro & ConsDocument8 pagesThrombolysis Pro & ConsSofia KusumadewiNo ratings yet
- Sinus Is It Always NormalDocument27 pagesSinus Is It Always NormalSofia KusumadewiNo ratings yet
- Evaluating Left Atrial Function in Mitral Valve DiseaseDocument30 pagesEvaluating Left Atrial Function in Mitral Valve DiseaseSofia KusumadewiNo ratings yet
- Pharmacological Therapy in Life Threatening ArrhythmiaDocument20 pagesPharmacological Therapy in Life Threatening ArrhythmiaSofia KusumadewiNo ratings yet
- Echocardiography For Systemic DiseaseDocument81 pagesEchocardiography For Systemic DiseaseSofia KusumadewiNo ratings yet
- When Will PVC For WS PDFDocument30 pagesWhen Will PVC For WS PDFSofia KusumadewiNo ratings yet
- Stress Echocardiography For Valvular Heart DiseaseDocument39 pagesStress Echocardiography For Valvular Heart DiseaseSofia KusumadewiNo ratings yet
- DIAGNOSTIC TOOL FOR CHEST PAIN SYMPTOM, Dr. BRM Ario Suryo SP - JP (K), FAsCC PDFDocument23 pagesDIAGNOSTIC TOOL FOR CHEST PAIN SYMPTOM, Dr. BRM Ario Suryo SP - JP (K), FAsCC PDFSofia KusumadewiNo ratings yet
- Principle and Practice of CT in Cardiac AssessmentDocument47 pagesPrinciple and Practice of CT in Cardiac AssessmentSofia KusumadewiNo ratings yet
- Eset Serial KeyDocument2 pagesEset Serial KeySofia Kusumadewi25% (4)
- Principle and Practice of Cardiac Mechanic For Assessing LV FunctionDocument33 pagesPrinciple and Practice of Cardiac Mechanic For Assessing LV FunctionSofia Kusumadewi100% (1)
- Current Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFDocument51 pagesCurrent Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFSofia KusumadewiNo ratings yet
- Edwin S. Tucay, MD Fpse Fascc: Noninvasive Cardiac Laboratory Philippine Heart CenterDocument36 pagesEdwin S. Tucay, MD Fpse Fascc: Noninvasive Cardiac Laboratory Philippine Heart CenterSofia KusumadewiNo ratings yet
- Echocardiography Evaluation For The Tricuspid ValveDocument48 pagesEchocardiography Evaluation For The Tricuspid ValveSofia KusumadewiNo ratings yet
- DIAGNOSTIC TOOL FOR CHEST PAIN SYMPTOM, Dr. BRM Ario Suryo SP - JP (K), FAsCC PDFDocument23 pagesDIAGNOSTIC TOOL FOR CHEST PAIN SYMPTOM, Dr. BRM Ario Suryo SP - JP (K), FAsCC PDFSofia KusumadewiNo ratings yet
- Diastolic Stress Echocardiography PDFDocument23 pagesDiastolic Stress Echocardiography PDFSofia KusumadewiNo ratings yet
- Current Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFDocument51 pagesCurrent Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFSofia KusumadewiNo ratings yet
- Sign Symptom AdultchdDocument13 pagesSign Symptom AdultchdSofia KusumadewiNo ratings yet
- Management VTEDocument48 pagesManagement VTEsofiNo ratings yet
- Dr. Hasanah DX Op PH - JCU 18 Simpo - DR HM PDFDocument36 pagesDr. Hasanah DX Op PH - JCU 18 Simpo - DR HM PDFSofia KusumadewiNo ratings yet
- Dr. Hasanah DX Op PH - JCU 18 Simpo - DR HM PDFDocument36 pagesDr. Hasanah DX Op PH - JCU 18 Simpo - DR HM PDFSofia KusumadewiNo ratings yet
- Raharjo SB - JCU 2018 - Multimodality On Atrial FibrillationDocument37 pagesRaharjo SB - JCU 2018 - Multimodality On Atrial FibrillationSofia KusumadewiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GMDSSDocument1 pageGMDSSRahul rajeshNo ratings yet
- PresentationDocument6 pagesPresentationVruchali ThakareNo ratings yet
- MGN815: Business Models: Ajay ChandelDocument38 pagesMGN815: Business Models: Ajay ChandelSam RehmanNo ratings yet
- Project 2 Analysis of Florida WaterDocument8 pagesProject 2 Analysis of Florida WaterBeau Beauchamp100% (1)
- PCZ 1503020 CeDocument73 pagesPCZ 1503020 Cedanielradu27No ratings yet
- Kübra Şendoğan CVDocument5 pagesKübra Şendoğan CVKübra ŞendoğanNo ratings yet
- HP 6940 Manual CompleteDocument150 pagesHP 6940 Manual CompletepaglafouNo ratings yet
- Summer Internship Project Report ANALYSIDocument60 pagesSummer Internship Project Report ANALYSIKshitija KudacheNo ratings yet
- The Role of IT in TQM L'Oreal Case StudyDocument9 pagesThe Role of IT in TQM L'Oreal Case StudyUdrea RoxanaNo ratings yet
- Couvade SyndromeDocument5 pagesCouvade SyndromejudssalangsangNo ratings yet
- Encephalopathies: Zerlyn T. Leonardo, M.D., FPCP, FPNADocument50 pagesEncephalopathies: Zerlyn T. Leonardo, M.D., FPCP, FPNAJanellee DarucaNo ratings yet
- Ahu 1997 22 1 95Document15 pagesAhu 1997 22 1 95Pasajera En TranceNo ratings yet
- Fuel SystemDocument24 pagesFuel SystemHammad Uddin JamilyNo ratings yet
- An Enhanced RFID-Based Authentication Protocol Using PUF For Vehicular Cloud ComputingDocument18 pagesAn Enhanced RFID-Based Authentication Protocol Using PUF For Vehicular Cloud Computing0dayNo ratings yet
- Dosificación Gac007-008 Sem2Document2 pagesDosificación Gac007-008 Sem2Ohm EgaNo ratings yet
- BPI - I ExercisesDocument241 pagesBPI - I Exercisesdivyajeevan89No ratings yet
- Probset 3 KeyDocument7 pagesProbset 3 KeyhoneyschuNo ratings yet
- On The Margins - A Study of The Experiences of Transgender College StudentsDocument14 pagesOn The Margins - A Study of The Experiences of Transgender College StudentsRory J. BlankNo ratings yet
- Procedure Manual - IMS: Locomotive Workshop, Northern Railway, LucknowDocument8 pagesProcedure Manual - IMS: Locomotive Workshop, Northern Railway, LucknowMarjorie Dulay Dumol80% (5)
- Ethernet: Outline Multiple Access and Ethernet Intro Ethernet Framing CSMA/CD Protocol Exponential BackoffDocument25 pagesEthernet: Outline Multiple Access and Ethernet Intro Ethernet Framing CSMA/CD Protocol Exponential BackoffcheckNo ratings yet
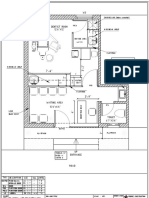
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- CHAPTER THREE-Teacher's PetDocument3 pagesCHAPTER THREE-Teacher's PetTaylor ComansNo ratings yet
- Introduction To Cobit Framework - Week 3Document75 pagesIntroduction To Cobit Framework - Week 3Teddy HaryadiNo ratings yet
- Norm ANSI PDFDocument1 pageNorm ANSI PDFAbdul Quddus Mat IsaNo ratings yet
- Practical Research 2 Group 11 RRL, Proposed Title and Answers To The QuestionsDocument14 pagesPractical Research 2 Group 11 RRL, Proposed Title and Answers To The QuestionsFeby Margaret AngNo ratings yet
- Solutions - HW 3, 4Document5 pagesSolutions - HW 3, 4batuhany90No ratings yet
- ARRANGING For Marchong or Concert BandDocument13 pagesARRANGING For Marchong or Concert BandCheGus AtilanoNo ratings yet
- Sheridan Specialized Building Products LLC - Queue Solutions Commercial Proposal by SeQure TechnologiesDocument6 pagesSheridan Specialized Building Products LLC - Queue Solutions Commercial Proposal by SeQure Technologiessailesh psNo ratings yet
- Heart Attack Detection ReportDocument67 pagesHeart Attack Detection ReportAkhil TejaNo ratings yet
- What Role Does Imagination Play in Producing Knowledge About The WorldDocument1 pageWhat Role Does Imagination Play in Producing Knowledge About The WorldNathanael Samuel KuruvillaNo ratings yet