You might also like
- Current Therapeutic Advances in Chronic Interstitial CystitisDocument8 pagesCurrent Therapeutic Advances in Chronic Interstitial CystitisYylfordt GranzNo ratings yet
- Diarrhea During Critical Illness A Multicenter PDFDocument10 pagesDiarrhea During Critical Illness A Multicenter PDFRejanne OliveiraNo ratings yet
- Etiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisDocument8 pagesEtiology and Risk Factors of Acute Gastroenteritis in A Taipei Emergency Department: Clinical Features For Bacterial GastroenteritisakhmadNo ratings yet
- JJZ 203Document1 pageJJZ 203Juan DiegoNo ratings yet
- 12076Document7 pages12076Muhammad ZiaNo ratings yet
- Alkaline IBSDocument9 pagesAlkaline IBSAnh LevanNo ratings yet
- Diarrea en Enfermedad CríticaDocument10 pagesDiarrea en Enfermedad CríticaVíctor Pérez RiveroNo ratings yet
- Effect of Vitamin D Supplementation on Primary Dysmenorrhea A Systematic Reviewand Meta-Analysis of Randomized Clinical TrialsDocument15 pagesEffect of Vitamin D Supplementation on Primary Dysmenorrhea A Systematic Reviewand Meta-Analysis of Randomized Clinical TrialsFransiska FranshuidNo ratings yet
- Efficacy of Early Immunomodulator Therapy On The Outcomes of Crohn 'S DiseaseDocument6 pagesEfficacy of Early Immunomodulator Therapy On The Outcomes of Crohn 'S Diseasehusni gunawanNo ratings yet
- Perri2003 PDFDocument8 pagesPerri2003 PDFnageshkamatNo ratings yet
- D Yspepsia and Helicobacter Pylori Infection: A Prospective Multicentre Observational StudyDocument8 pagesD Yspepsia and Helicobacter Pylori Infection: A Prospective Multicentre Observational StudynageshkamatNo ratings yet
- ContentServer - Asp 13Document7 pagesContentServer - Asp 13Fitria NurulfathNo ratings yet
- A Study On Acute Surgical Abdomen in Paediatric Age Group: Original Research ArticleDocument5 pagesA Study On Acute Surgical Abdomen in Paediatric Age Group: Original Research ArticleApple IdeaNo ratings yet
- Paper 26Document4 pagesPaper 26fundj22No ratings yet
- Title An Audit of Microbiological Tests in A Primary Care ClinicDocument20 pagesTitle An Audit of Microbiological Tests in A Primary Care ClinicHam FGNo ratings yet
- 2022_lingyu_Acupuncture for the Treatment of Diarrhea-Predominant_ecaDocument11 pages2022_lingyu_Acupuncture for the Treatment of Diarrhea-Predominant_ecaesmargarNo ratings yet
- Sii ArtículoDocument5 pagesSii ArtículoMonserrat Garduño FonsecaNo ratings yet
- 11111111Document7 pages11111111Nejc KovačNo ratings yet
- Clinical Outcomes of Esophagogastroduodenoscopy In.27Document6 pagesClinical Outcomes of Esophagogastroduodenoscopy In.27Agung KaryawinaraNo ratings yet
- Appendicitis Clinical Pathway Implementations Compliance Evaluation in HospitalDocument4 pagesAppendicitis Clinical Pathway Implementations Compliance Evaluation in HospitalsuriNo ratings yet
- The Role of Drotaverine in IbsDocument5 pagesThe Role of Drotaverine in IbsAli Abd AlrezaqNo ratings yet
- Madisch Treatment of Irritable Bowel Syndrome With Herbal PreparationsDocument9 pagesMadisch Treatment of Irritable Bowel Syndrome With Herbal Preparationsoliffasalma atthahirohNo ratings yet
- Upadacitinib Treatment Improves Symptoms of Bowel Urgency and Abdominal Pain, and Correlates With Quality of Life Improvements in Patients With Moderate To Severe Ulcerative ColitisDocument9 pagesUpadacitinib Treatment Improves Symptoms of Bowel Urgency and Abdominal Pain, and Correlates With Quality of Life Improvements in Patients With Moderate To Severe Ulcerative Colitisslt.hi468No ratings yet
- ITU Comparacion 7 - 14 Dias de TtoDocument9 pagesITU Comparacion 7 - 14 Dias de TtoJohana Zamudio RojasNo ratings yet
- 10 1016@j Ejogrb 2015 09 020Document5 pages10 1016@j Ejogrb 2015 09 020samuel tapia pardoNo ratings yet
- Acupuncture Treatment in Gastrointestinal Diseases: A Systematic ReviewDocument8 pagesAcupuncture Treatment in Gastrointestinal Diseases: A Systematic ReviewVicTör Manuel Apölo-ğNo ratings yet
- Chen. M SR and Three Level MADocument17 pagesChen. M SR and Three Level MASreeja CherukuruNo ratings yet
- A Randomized Controlled Trial of Probiotics For Clostridium Dif Cile Infection in AdultsDocument4 pagesA Randomized Controlled Trial of Probiotics For Clostridium Dif Cile Infection in Adults林新中No ratings yet
- The Effects of Abdominal I LOV U Massage Along With Lifestyle Training On Constipation and Distension in The Elderly With StrokeDocument9 pagesThe Effects of Abdominal I LOV U Massage Along With Lifestyle Training On Constipation and Distension in The Elderly With StrokeSuci NudiNo ratings yet
- Alvorado ComparingDocument8 pagesAlvorado ComparingHarun NasutionNo ratings yet
- Leaflet Preeklamsia BeratDocument6 pagesLeaflet Preeklamsia BeratSafitriNo ratings yet
- Acyclovir Treatment Efficacy in Pemphigus VulgarisDocument3 pagesAcyclovir Treatment Efficacy in Pemphigus Vulgarissuci sukmawatiNo ratings yet
- SIBO EritromicinaDocument8 pagesSIBO EritromicinaKat HerreraNo ratings yet
- 1,2,Document11 pages1,2,Nejc KovačNo ratings yet
- Trial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionDocument10 pagesTrial of Short-Course Antimicrobial Therapy For Intraabdominal InfectionMeygan CórdovaNo ratings yet
- Fit and Fecal Calprotectin 2020Document6 pagesFit and Fecal Calprotectin 2020sashadilanNo ratings yet
- Multiplex Gastrointestinal Pentru ClinicieniDocument2 pagesMultiplex Gastrointestinal Pentru ClinicieniNadiNo ratings yet
- 1471 230X 7 9 PDFDocument5 pages1471 230X 7 9 PDFivanhariachandraNo ratings yet
- 2022 JastreboffDocument12 pages2022 JastreboffSinityNo ratings yet
- Chen 2021Document8 pagesChen 2021metha anandaNo ratings yet
- Enteral Nutrition Therapy For The Surgical PatientDocument52 pagesEnteral Nutrition Therapy For The Surgical PatientelenNo ratings yet
- Research Paper Effectiveness of Conservative Management of Uncomplicated Acute Appendicitis: A Single Hospital Based Prospective StudyDocument8 pagesResearch Paper Effectiveness of Conservative Management of Uncomplicated Acute Appendicitis: A Single Hospital Based Prospective StudyAnsoriNo ratings yet
- Short-Course Intraabdominal InfectionDocument10 pagesShort-Course Intraabdominal Infectionnicolás idárragaNo ratings yet
- Effectiveness of Acupuncture in The Treatment of Hyperemesis Gravidarum - A Systematic Review and Meta-AnalysisDocument14 pagesEffectiveness of Acupuncture in The Treatment of Hyperemesis Gravidarum - A Systematic Review and Meta-Analysiswiwit vitaniaNo ratings yet
- Ramirez 2013Document10 pagesRamirez 2013Nadia Farah FadhilaNo ratings yet
- A Double Blind, Randomised, Placebo-Controlled Trial of Lactobacillus Acute Watery Diarrhoea in Vietnamese ChildrenDocument26 pagesA Double Blind, Randomised, Placebo-Controlled Trial of Lactobacillus Acute Watery Diarrhoea in Vietnamese ChildrenSeftiyantiNo ratings yet
- FDA Approves Lilly's Omvoh - (Mirikizumab-Mrkz), A First-in-Class Treatment For Adults With Moderately To Severely Active Ulcerative ColitisDocument4 pagesFDA Approves Lilly's Omvoh - (Mirikizumab-Mrkz), A First-in-Class Treatment For Adults With Moderately To Severely Active Ulcerative ColitisOscar OrtegaNo ratings yet
- Art 21054Document10 pagesArt 21054Ndhy Pharm HabibieNo ratings yet
- El Tratamiento de La Obstrucción Del Intestino Delgado Con Un Fisioterapia Manual - Un Estudio de Eficacia Prospectivo.Document10 pagesEl Tratamiento de La Obstrucción Del Intestino Delgado Con Un Fisioterapia Manual - Un Estudio de Eficacia Prospectivo.DanielaNo ratings yet
- 1741 7015 8 30Document8 pages1741 7015 8 30Andres HernándezNo ratings yet
- Jurnal Jaki Prof VeniDocument38 pagesJurnal Jaki Prof Veniiman prawiraNo ratings yet
- Clinical Effect of Catgut Implantation at AcupointsDocument8 pagesClinical Effect of Catgut Implantation at AcupointsJuan Pablo MejíaNo ratings yet
- Bet 6 300Document6 pagesBet 6 300Victor SanchezNo ratings yet
- Pi Is 0016508520300184Document12 pagesPi Is 0016508520300184ntnquynhproNo ratings yet
- Abcesele FicatuluiDocument4 pagesAbcesele FicatuluiMihaela AlinaNo ratings yet
- 5 02 Acute Abdominal PainDocument17 pages5 02 Acute Abdominal PainNereida LechugaNo ratings yet
- CosentyxDocument10 pagesCosentyxsamar RamadanNo ratings yet
- Jour Red UrticariaDocument6 pagesJour Red UrticariaErianaSariNo ratings yet
- Critical Care II Nutrition Support Team EvaluationDocument1 pageCritical Care II Nutrition Support Team EvaluationWilma Maria Coelho AraujoNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 5: GastrointestinalFrom EverandComplementary and Alternative Medical Lab Testing Part 5: GastrointestinalNo ratings yet
- Jurnal MH PDFDocument12 pagesJurnal MH PDFcamelia musaadNo ratings yet
- Resources Used in This Design Url: Background - 3956685.htmDocument1 pageResources Used in This Design Url: Background - 3956685.htmcamelia musaadNo ratings yet
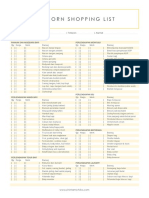
- Newborn Shopping List TemplateDocument1 pageNewborn Shopping List TemplateShellaCharismaAgryanandhaNo ratings yet
- Jurnal Ebm KedkelDocument8 pagesJurnal Ebm Kedkelcamelia musaadNo ratings yet
- Ebm JurnalDocument198 pagesEbm Jurnalcamelia musaadNo ratings yet
- Referat Asma AnakDocument26 pagesReferat Asma Anakcamelia musaadNo ratings yet
- kjr-US For Benign and Maligna PDFDocument9 pageskjr-US For Benign and Maligna PDFLiaNo ratings yet
- Surat Sponsor 1Document1 pageSurat Sponsor 1camelia musaadNo ratings yet
- Ebm Jurnal PDFDocument198 pagesEbm Jurnal PDFcamelia musaadNo ratings yet
- Surat Pernyataaan NPWPDocument1 pageSurat Pernyataaan NPWPcamelia musaadNo ratings yet
- Management of Abcess CerebriDocument6 pagesManagement of Abcess Cerebricamelia musaadNo ratings yet
- Brain Abscess in ChildrenDocument5 pagesBrain Abscess in Childrencamelia musaadNo ratings yet
- Brain Abscess: H. R W, M.DDocument1 pageBrain Abscess: H. R W, M.Dcamelia musaadNo ratings yet
- Epid, MK, ManagementDocument4 pagesEpid, MK, Managementcamelia musaadNo ratings yet
- Jean Elizabeth HamptonDocument3 pagesJean Elizabeth HamptonTamannaNo ratings yet
- Jurisidiction of MeTC, MTC, MCTC, MuTCDocument3 pagesJurisidiction of MeTC, MTC, MCTC, MuTCKENEDY FLORESNo ratings yet
- Person On The StreetDocument12 pagesPerson On The StreetalyssajdorazioNo ratings yet
- Timeline of The Human SocietyDocument3 pagesTimeline of The Human SocietyAtencio Barandino JhonilNo ratings yet
- DeKalb Pay Raise Summary July 6 2022Document8 pagesDeKalb Pay Raise Summary July 6 2022Janet and JamesNo ratings yet
- LightingDocument157 pagesLightingtalibanindonesiaNo ratings yet
- Human Resource Strategy: Atar Thaung HtetDocument16 pagesHuman Resource Strategy: Atar Thaung HtetaungnainglattNo ratings yet
- Strategy Map - Visualize Goals & ObjectivesDocument22 pagesStrategy Map - Visualize Goals & ObjectivesNitin JainNo ratings yet
- Ssees DissertationDocument5 pagesSsees DissertationBuyAcademicPapersCanada100% (1)
- Report Daftar Penerima Kuota Telkomsel Dan Indosat 2021 FSEIDocument26 pagesReport Daftar Penerima Kuota Telkomsel Dan Indosat 2021 FSEIHafizh ZuhdaNo ratings yet
- Techno ReadDocument11 pagesTechno ReadCelrose FernandezNo ratings yet
- Grade 8 Lesson on "The Filipino is Worth Dying ForDocument5 pagesGrade 8 Lesson on "The Filipino is Worth Dying ForHanna ManiteNo ratings yet
- Calendar of ActivitiesDocument7 pagesCalendar of ActivitiesAries Robinson CasasNo ratings yet
- Sector:: Automotive/Land Transport SectorDocument20 pagesSector:: Automotive/Land Transport SectorVedin Padilla Pedroso92% (12)
- SF3 - 2022 - Grade 8 SAMPLEDocument2 pagesSF3 - 2022 - Grade 8 SAMPLEANEROSE DASIONNo ratings yet
- Cityam 2011-09-19Document36 pagesCityam 2011-09-19City A.M.No ratings yet
- EMship Course ContentDocument82 pagesEMship Course ContentBecirspahic Almir100% (1)
- Writing Essays B1Document6 pagesWriting Essays B1Manuel Jose Arias TabaresNo ratings yet
- Numerology Speaking PDFDocument7 pagesNumerology Speaking PDFValeria NoginaNo ratings yet
- Dentsply Sirona Q2 Earnings Presentation - FINALDocument18 pagesDentsply Sirona Q2 Earnings Presentation - FINALmedtechyNo ratings yet
- Sermon 7 - Friendship and Fellowship of The Gospel - Part 6 - Philemon 7Document32 pagesSermon 7 - Friendship and Fellowship of The Gospel - Part 6 - Philemon 7Rob WilkersonNo ratings yet
- Assignment 1Document3 pagesAssignment 1Rabia Ahmad100% (1)
- Shukr Thankfulness To Allah Grade 12Document21 pagesShukr Thankfulness To Allah Grade 12Salman Mohammed AbdullahNo ratings yet
- Dissertation Le Juge Administratif Et Le Droit InternationalDocument8 pagesDissertation Le Juge Administratif Et Le Droit InternationalPayPeopleToWritePapersWestValleyCityNo ratings yet
- HPLC Method for Simultaneous Determination of DrugsDocument7 pagesHPLC Method for Simultaneous Determination of DrugsWidya Dwi Arini100% (1)
- Physiotherapy's Role in Rehabilitation and Health Promotion Across the LifespanDocument3 pagesPhysiotherapy's Role in Rehabilitation and Health Promotion Across the LifespanMariana OspinaNo ratings yet
- Pro ManualDocument67 pagesPro ManualAlan De La FuenteNo ratings yet
- Tiếng Anh 6 Smart World - Unit 10 - CITIES AROUND THE WORLD - SBDocument33 pagesTiếng Anh 6 Smart World - Unit 10 - CITIES AROUND THE WORLD - SBponyoNo ratings yet
- Speakout E3 B1+ U2 - Teachers BookDocument20 pagesSpeakout E3 B1+ U2 - Teachers BookCarolinaNo ratings yet
- Practices For Improving The PCBDocument35 pagesPractices For Improving The PCBmwuestNo ratings yet