You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Large, Solitary, Luteinized Follicle Cyst of Pregnancy and PuerperiumDocument5 pagesLarge, Solitary, Luteinized Follicle Cyst of Pregnancy and PuerperiumMade RusmanaNo ratings yet
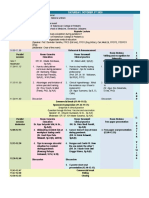
- Agenda Postgradmededu 120920 PDFDocument2 pagesAgenda Postgradmededu 120920 PDFStella NoviaNo ratings yet
- 04 Boys Bbu 05tDocument2 pages04 Boys Bbu 05tMauLan SaputraNo ratings yet
- Time (Wita) Saturday, October 3 2020Document2 pagesTime (Wita) Saturday, October 3 2020Made RusmanaNo ratings yet
- Large Luteinized Follicular Cyst of Pregnancy: G. Mavromatidis, A. Sotiriadis, K. Dinas, A. Mamopoulos and D. RoussoDocument4 pagesLarge Luteinized Follicular Cyst of Pregnancy: G. Mavromatidis, A. Sotiriadis, K. Dinas, A. Mamopoulos and D. RoussoMade RusmanaNo ratings yet
- Agenda Postgradmededu 120920 PDFDocument2 pagesAgenda Postgradmededu 120920 PDFStella NoviaNo ratings yet
- Rundown PIT IAPIDocument2 pagesRundown PIT IAPIMade RusmanaNo ratings yet
- 2021 Publication Case Report - Frontal MucoceleDocument3 pages2021 Publication Case Report - Frontal MucoceleMade RusmanaNo ratings yet
- Who PeritoneumDocument2 pagesWho PeritoneumMade RusmanaNo ratings yet
- Who Ovary1Document5 pagesWho Ovary1Made RusmanaNo ratings yet
- Who Classification of Tumours of The VulvaDocument3 pagesWho Classification of Tumours of The VulvaMade RusmanaNo ratings yet
- Thy 2015 0020 PDFDocument271 pagesThy 2015 0020 PDFMade RusmanaNo ratings yet
- Thy 2015 0020 PDFDocument271 pagesThy 2015 0020 PDFMade RusmanaNo ratings yet
- Thy 2015 0020 PDFDocument271 pagesThy 2015 0020 PDFMade RusmanaNo ratings yet
- Thyroid Ca MortalityDocument9 pagesThyroid Ca MortalityMade RusmanaNo ratings yet
- BRAFV600E Mutation Is Associated With Tumor AggressivenessDocument8 pagesBRAFV600E Mutation Is Associated With Tumor AggressivenessMade RusmanaNo ratings yet
- AssociationBetweenBRAFV600EMutationand MortalityDocument9 pagesAssociationBetweenBRAFV600EMutationand MortalityMade RusmanaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Human Excretory SystemDocument2 pagesHuman Excretory SystemVio ElenaNo ratings yet
- 7th Class Science-SEM2Document208 pages7th Class Science-SEM2Vishnu Vijay shankarNo ratings yet
- Biology Unit 6 Study Guide AnswersDocument3 pagesBiology Unit 6 Study Guide AnswersmisterbrownerNo ratings yet
- Anti HIV Using Nanorobots: Dr. Ankita Joshi, Akash PardeshiDocument7 pagesAnti HIV Using Nanorobots: Dr. Ankita Joshi, Akash PardeshiAmal Rejan Amal RejanNo ratings yet
- Aakash Botany Study Package 4 SolutionssssDocument120 pagesAakash Botany Study Package 4 SolutionssssRishika PaulNo ratings yet
- Plant Symbionts InteractionDocument13 pagesPlant Symbionts InteractionIram TahirNo ratings yet
- DISORDERS AND DISEASES CELL CYCLE - EllaDocument9 pagesDISORDERS AND DISEASES CELL CYCLE - EllaKennedy Fieldad Vagay100% (1)
- Pharmacoinformatics: A Tool For Drug DiscoveryDocument29 pagesPharmacoinformatics: A Tool For Drug Discoveryahirebhupendra100% (1)
- PlanktonDocument12 pagesPlanktonRen ObeñaNo ratings yet
- Monera - WikipediaDocument46 pagesMonera - WikipediaBashiir NuurNo ratings yet
- The Importance of Health Fitness and WellnessDocument3 pagesThe Importance of Health Fitness and Wellnessapi-25954769No ratings yet
- Cytogenetics Transes Topic 16Document5 pagesCytogenetics Transes Topic 16Dianne NolascoNo ratings yet
- Storing Bacterial Samples For Optimal Viability - Thermo Fisher Scientific - IDDocument3 pagesStoring Bacterial Samples For Optimal Viability - Thermo Fisher Scientific - IDoktaNo ratings yet
- Cell - Structure and Functions: World of CellsDocument5 pagesCell - Structure and Functions: World of CellsPriyanshu Priyadarshi MeherNo ratings yet
- 71 Questions of Importance For Marine Conservation (ParsonsFavaro - Etal - 2014) PDFDocument10 pages71 Questions of Importance For Marine Conservation (ParsonsFavaro - Etal - 2014) PDFRoky Mountains HillNo ratings yet
- Elife 05826Document12 pagesElife 05826Ema GuillotineNo ratings yet
- Darwin Among The MachinesDocument5 pagesDarwin Among The Machinesoliv_silv100% (2)
- Time Secrets of Living LongerDocument108 pagesTime Secrets of Living Longeraramisbirsan2132No ratings yet
- Green BiotechnologyDocument7 pagesGreen BiotechnologyDhirajNo ratings yet
- Fermentation FundamentalsDocument5 pagesFermentation FundamentalsWade ColemanNo ratings yet
- Lesson Plan On EubacteriaDocument3 pagesLesson Plan On Eubacteriajacquelyn celestialNo ratings yet
- PG BookDocument5 pagesPG BookUnnithan Rendezvous100% (2)
- CauveryMK - CVDocument3 pagesCauveryMK - CVMichelle KnightNo ratings yet
- Biodiversity of Flora and FaunaDocument13 pagesBiodiversity of Flora and FaunaLasmaenita SiahaanNo ratings yet
- Zone Diet: What Is The Zone?Document10 pagesZone Diet: What Is The Zone?Julyan FelizNo ratings yet
- The Digestive System MODULEDocument3 pagesThe Digestive System MODULEBen Moldenhaur100% (2)
- Stuck and Sluggish FermentationsDocument13 pagesStuck and Sluggish Fermentations1ab4cNo ratings yet
- HSA. Past Papers With Answer SDocument33 pagesHSA. Past Papers With Answer SAaron Baker100% (1)
- 2011 Fractal DNADocument7 pages2011 Fractal DNAAbby SweeneyNo ratings yet
- Boon or BaneDocument5 pagesBoon or BanesujeeNo ratings yet