You might also like
- Psychiatric NursingDocument21 pagesPsychiatric NursingFreeNursingNotes92% (38)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Kerry Layne Author Albert Ferro Author 100 Cases in Clinical PharmacologyDocument249 pagesKerry Layne Author Albert Ferro Author 100 Cases in Clinical Pharmacologyteju100% (3)
- 101 Ways To Improve Customer ServiceDocument398 pages101 Ways To Improve Customer ServiceSeto WibowoNo ratings yet
- Pharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDocument5 pagesPharmacology - Use of Beta-Blockers & Arbs in Cardiovascular Disease Treating HypertensionDana20SNo ratings yet
- Drugclasses Pharmacologypart 1 PDFDocument25 pagesDrugclasses Pharmacologypart 1 PDFSutanya100% (2)
- Medics PHC Protocols 3rd EditionDocument102 pagesMedics PHC Protocols 3rd EditionLee HillNo ratings yet
- Fluid Overload Student PagesDocument4 pagesFluid Overload Student PagesJess OswaldNo ratings yet
- Kchristman Maltol Extraction and Purification Report 2Document6 pagesKchristman Maltol Extraction and Purification Report 2api-694290335100% (1)
- Infection of The Skin, Soft Tissue, Etc.Document84 pagesInfection of The Skin, Soft Tissue, Etc.fmds100% (1)
- Medication DilutionDocument23 pagesMedication DilutionamgdanielaNo ratings yet
- IR IntroductionDocument48 pagesIR IntroductionMuhammad Erik Rezakola Ahnaf100% (1)
- Classification of The DrugsDocument50 pagesClassification of The DrugsGlena SalamNo ratings yet
- Pharm C Exam 10 Drug ListDocument2 pagesPharm C Exam 10 Drug ListVokdadaNo ratings yet
- Liposomal IronDocument6 pagesLiposomal IronPiyush KhetrapalNo ratings yet
- Ferosac InjDocument2 pagesFerosac InjMohamed Taleb75% (4)
- Coral CalciumDocument6 pagesCoral Calciumfariha farheenNo ratings yet
- Behavioral Interviewing Guide For Early Career Candidates PDFDocument97 pagesBehavioral Interviewing Guide For Early Career Candidates PDFClaudia ȚirbanNo ratings yet
- OsteoporosisDocument19 pagesOsteoporosisLasa SiahaanNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument51 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsClaudia TiffanyNo ratings yet
- 2014 Leaflet Dosage High-Resolution-1Document4 pages2014 Leaflet Dosage High-Resolution-1Zarbakht AliNo ratings yet
- Conventional Drug Delivery Routes, Recent Developments and Future Prospects - Tugas SPO "Document21 pagesConventional Drug Delivery Routes, Recent Developments and Future Prospects - Tugas SPO "Niken Dwi100% (1)
- Pharmacology Module PDFDocument23 pagesPharmacology Module PDFmirza_baig_46100% (1)
- Iron Deficiency Anemia PDFDocument61 pagesIron Deficiency Anemia PDFbhat Library100% (1)
- Mini RinDocument5 pagesMini Rinlovely_dyaNo ratings yet
- Pi Is 1548559519301144Document20 pagesPi Is 1548559519301144hemer hadyn calderon alvites0% (1)
- Liposomes: Controlled Delivery SystemsDocument31 pagesLiposomes: Controlled Delivery SystemsDRx Sonali Tarei100% (1)
- Drug Study of 10-Year-Old Girl with DengueDocument3 pagesDrug Study of 10-Year-Old Girl with DengueJuliane ItliongNo ratings yet
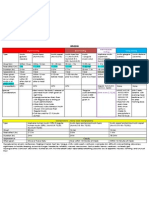
- Drug Classificati On Indications Action Route/Dos e Side Effects Patient Teaching Nursing ImplicationsDocument7 pagesDrug Classificati On Indications Action Route/Dos e Side Effects Patient Teaching Nursing ImplicationsJenny NguyenNo ratings yet
- Administering Vaccines To AdultsDocument1 pageAdministering Vaccines To AdultsPaul Anthony LoricaNo ratings yet
- Common Prefixes and SuffixesDocument5 pagesCommon Prefixes and Suffixestriddle1969100% (1)
- (Pha) Le 5Document19 pages(Pha) Le 5Gabby TanNo ratings yet
- Dka Guidelines - 2012Document4 pagesDka Guidelines - 2012djizhieeNo ratings yet
- PG PREPARATION - Mnemonics in PharmacologyDocument12 pagesPG PREPARATION - Mnemonics in PharmacologyRaveen KumarNo ratings yet
- Drug CardsDocument3 pagesDrug CardsDave HillNo ratings yet
- Drug of Abuse (Table) PDFDocument2 pagesDrug of Abuse (Table) PDFtchanochNo ratings yet
- Drug Compatibility in Intravenous Y-Site AdministrationDocument4 pagesDrug Compatibility in Intravenous Y-Site Administrationtuti haryatiNo ratings yet
- List of Look-Alike MedicationsDocument5 pagesList of Look-Alike MedicationsAhmad TaramsyNo ratings yet
- Pharm Expansion 17 NDFDocument1 pagePharm Expansion 17 NDFNokz M. Raki-inNo ratings yet
- Drug Classes and Brand NamesDocument6 pagesDrug Classes and Brand Namesremyde07No ratings yet
- Assay For Citric AcidDocument3 pagesAssay For Citric AcidLRahmawNo ratings yet
- Pharmacopeia 1 (Autosaved)Document12 pagesPharmacopeia 1 (Autosaved)farooq shah shabbirNo ratings yet
- Transport of Critically Ill Adults 2011Document1 pageTransport of Critically Ill Adults 2011velocity25No ratings yet
- Drugs in Blood DisordersDocument1 pageDrugs in Blood DisordersSantosh patelNo ratings yet
- Enve 208 Experiment 2.1 SonDocument10 pagesEnve 208 Experiment 2.1 Sonmihrican302No ratings yet
- Amino Acid Analysis Using ZORBAX Eclipse AAA ColumnsDocument10 pagesAmino Acid Analysis Using ZORBAX Eclipse AAA ColumnsMuhammad KhairulnizamNo ratings yet
- CAL GluconateDocument29 pagesCAL Gluconatehumag143100% (1)
- Iron Deficiency AnemiaDocument12 pagesIron Deficiency AnemiaFeraNoviantiNo ratings yet
- Insulin Chart 05032012 PDFDocument1 pageInsulin Chart 05032012 PDFTiffany CrittendenNo ratings yet
- Therapeutic IndexDocument8 pagesTherapeutic IndexMary Jennel RosNo ratings yet
- Combined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDDocument1 pageCombined Hormone Pill, Patch, Ring Progestin Only Mini Pill, Depo-Provera, IUDnkuligowskiNo ratings yet
- Experiment Estimation of Amino Acids: StructureDocument3 pagesExperiment Estimation of Amino Acids: StructureMàrwå Rägb ZäkyNo ratings yet
- Magnesium Oxide USP Monograph AnalysisDocument2 pagesMagnesium Oxide USP Monograph AnalysisIfra AkhlaqNo ratings yet
- L-Ornithine L-Aspartate For The Treatment of SarcopeniaDocument7 pagesL-Ornithine L-Aspartate For The Treatment of SarcopeniaNabeel Ahmed KhanNo ratings yet
- Drugs SummaryDocument23 pagesDrugs Summaryapi-3832811100% (1)
- Protein Calorie MalnutritionDocument97 pagesProtein Calorie Malnutritionnshaikh56No ratings yet
- Infrared Theory PDFDocument9 pagesInfrared Theory PDFATNo ratings yet
- KDOQI BoneGuide PDFDocument11 pagesKDOQI BoneGuide PDFAnna DangNo ratings yet
- Drugs Acting On The Blood and The BloodDocument26 pagesDrugs Acting On The Blood and The BloodHealthy7No ratings yet
- An Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFDocument6 pagesAn Easy Guide To Head To Toe Assessment Vrtis 2011-1 PDFkatherine dayagNo ratings yet
- Anti Anemia DrugsDocument36 pagesAnti Anemia DrugsArabelle GONo ratings yet
- Dissolution MethodsDocument216 pagesDissolution MethodsPUBG MOBILE - FANS CLUBNo ratings yet
- Medications Containing Alcohol and Options Without AlcoholDocument4 pagesMedications Containing Alcohol and Options Without AlcoholDikshit KapilaNo ratings yet
- Clinical Case Aki Presentation EportfolioDocument32 pagesClinical Case Aki Presentation Eportfolioapi-463444835No ratings yet
- Administering Vaccines: Dose, Route, Site and Needle Size GuideDocument1 pageAdministering Vaccines: Dose, Route, Site and Needle Size GuideKate Lucernas MayugaNo ratings yet
- Pharmacology of Drugs For AnemiaDocument49 pagesPharmacology of Drugs For AnemiaTeus Fatamorgana100% (2)
- AOE - Hiral Labs LTD Company Brochure 20180416170521Document20 pagesAOE - Hiral Labs LTD Company Brochure 20180416170521Dr VENKAT1 LUNo ratings yet
- The Leukotrienes: Chemistry and BiologyFrom EverandThe Leukotrienes: Chemistry and BiologyLawrence ChakrinNo ratings yet
- Management of Anaemia in PregnancyDocument8 pagesManagement of Anaemia in PregnancyAnonymous 9dVZCnTXSNo ratings yet
- See Full Prescribing Information For Complete Boxed WarningDocument53 pagesSee Full Prescribing Information For Complete Boxed WarningMohammed shamiul ShahidNo ratings yet
- From anti-malarial to antibacterial: The development of quinolone antibioticsDocument35 pagesFrom anti-malarial to antibacterial: The development of quinolone antibioticsmirza_baig_46No ratings yet
- Ciprofloxacin A Success StoryDocument27 pagesCiprofloxacin A Success Storymirza_baig_46No ratings yet
- Prostaglandins & COX Pathway OverviewDocument34 pagesProstaglandins & COX Pathway Overviewmirza_baig_46No ratings yet
- BBIFAQs PDFDocument2 pagesBBIFAQs PDFmirza_baig_46No ratings yet
- Gastroduodenal Mucus-Bicarbonate BarrierDocument19 pagesGastroduodenal Mucus-Bicarbonate Barriermirza_baig_46No ratings yet
- ClinicumDocument8 pagesClinicummirza_baig_46No ratings yet
- Airway Smooth Muscle RelaxationDocument8 pagesAirway Smooth Muscle Relaxationmirza_baig_46No ratings yet
- Employee Retention StrategiesDocument14 pagesEmployee Retention Strategiesmirza_baig_46No ratings yet
- Brand's nutritional supplements product listDocument1 pageBrand's nutritional supplements product listmirza_baig_46No ratings yet
- Gastroduodenal Mucus-Bicarbonate BarrierDocument19 pagesGastroduodenal Mucus-Bicarbonate Barriermirza_baig_46No ratings yet
- DRAP Safety Alert On Proton Pump InhibitorsDocument7 pagesDRAP Safety Alert On Proton Pump Inhibitorsmirza_baig_46No ratings yet
- Acetaminophen Properties Clinical Uses and Adverse Effects PDFDocument218 pagesAcetaminophen Properties Clinical Uses and Adverse Effects PDFmirza_baig_46No ratings yet
- Anatomy of The Muscular System PDFDocument48 pagesAnatomy of The Muscular System PDFmirza_baig_46No ratings yet
- Busn218 ChartsDocument17 pagesBusn218 Chartsmirza_baig_46No ratings yet
- Adenosine ReceptorDocument53 pagesAdenosine Receptormirza_baig_46100% (1)
- Malaria Treatment Guidelines-2 ND Edition 2011Document210 pagesMalaria Treatment Guidelines-2 ND Edition 2011Kevins KhaembaNo ratings yet
- Cambridge International Certificate For Teachers and Trainers Syllabus PDFDocument40 pagesCambridge International Certificate For Teachers and Trainers Syllabus PDFmirza_baig_46100% (1)
- Highline Excel 2016 Class 07 Excel 2016 MAXIFS, MINIFS & IFS Functions For Conditional CalculationsDocument5 pagesHighline Excel 2016 Class 07 Excel 2016 MAXIFS, MINIFS & IFS Functions For Conditional CalculationseneNo ratings yet
- Ananthanarayan and Paniker S Textbook of MicrobiologyDocument672 pagesAnanthanarayan and Paniker S Textbook of MicrobiologyBalakrishnan MarappanNo ratings yet
- State of World Antibiotics - 2015 - FinalDocument84 pagesState of World Antibiotics - 2015 - FinalsudeepbNo ratings yet
- The Guide To AstrologyDocument135 pagesThe Guide To Astrologymirza_baig_46No ratings yet
- The Guide To AstrologyDocument135 pagesThe Guide To Astrologymirza_baig_46No ratings yet
- Treatment Guide For Homeopathy PDFDocument79 pagesTreatment Guide For Homeopathy PDFlghmshariNo ratings yet
- Medical Mnemonics TitleDocument13 pagesMedical Mnemonics Titlemirza_baig_46100% (1)
- Norovirus 201309101051579338Document3 pagesNorovirus 201309101051579338Jeeva maria GeorgeNo ratings yet
- Neonatal Air Leak Syndrome and The Role Of.3Document9 pagesNeonatal Air Leak Syndrome and The Role Of.3Claudia KosztelnikNo ratings yet
- Micro-503 - (T) - Course Outline and ScheduleDocument2 pagesMicro-503 - (T) - Course Outline and ScheduleUmer AliNo ratings yet
- AphasiaDocument8 pagesAphasiaapi-308647214No ratings yet
- Alopecia Areata in Covid 19 Case ReportDocument2 pagesAlopecia Areata in Covid 19 Case ReportAnti TjahyaNo ratings yet
- MdsDocument570 pagesMdsAgus SusantoNo ratings yet
- TVI Lesson PlanDocument6 pagesTVI Lesson PlanRobelle RelativoNo ratings yet
- Andrew Eastman Resume 3Document2 pagesAndrew Eastman Resume 3api-281509868No ratings yet
- Permanent PacemakerDocument24 pagesPermanent PacemakerAwais PanhwarNo ratings yet
- Management of Intraocular Foreign BodiesDocument7 pagesManagement of Intraocular Foreign BodiesdebbyNo ratings yet
- Diastema Closure PDFDocument5 pagesDiastema Closure PDFsimon yonathanNo ratings yet
- Keeping Abreast of Future Need - A Report Into The Growing Demand For Breast Care NursesDocument14 pagesKeeping Abreast of Future Need - A Report Into The Growing Demand For Breast Care NursesEmmaNo ratings yet
- Female Anatomy ExplainedDocument11 pagesFemale Anatomy ExplainedBARRIENTOS, RITCHELLE C.No ratings yet
- Gynzone TrainingDocument62 pagesGynzone TrainingMariana PinheiroNo ratings yet
- CKD Report PDF ResizeDocument110 pagesCKD Report PDF Resizeहुमागाँई शिशिरNo ratings yet
- 01 MynckeDocument10 pages01 MynckeIrina DesyatykhNo ratings yet
- DKA Protocol With Calculation SheetDocument7 pagesDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNo ratings yet
- 127 FullDocument9 pages127 FullCho HyumiNo ratings yet
- Cancer: Get A Cancer Cover of ' 20 Lakhs at Less Than ' 4 / DayDocument6 pagesCancer: Get A Cancer Cover of ' 20 Lakhs at Less Than ' 4 / DayUtsav J BhattNo ratings yet
- Barrier MethodDocument3 pagesBarrier MethodJaninaPatriciaBNo ratings yet
- EctopicDocument4 pagesEctopicAb Staholic BoiiNo ratings yet
- Piriformis SyndromeDocument6 pagesPiriformis SyndromeChân Mệnh Thiên TửNo ratings yet
- Vit A DeficiencyDocument27 pagesVit A DeficiencyNatnaelNo ratings yet
- Etiology of Allergic Contact DermatitisDocument5 pagesEtiology of Allergic Contact DermatitisChichi Dita VirllianaNo ratings yet
- Government and Private Hospitals in BhopalDocument3 pagesGovernment and Private Hospitals in BhopalDeepak Kumar RajakNo ratings yet