You might also like
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Keating 2010Document7 pagesKeating 2010DR. OSORIONo ratings yet
- Accepted - Manuscrip Anakt PDFDocument23 pagesAccepted - Manuscrip Anakt PDFMiftahNo ratings yet
- Cystic Fibrosis: A DeconstructionDocument30 pagesCystic Fibrosis: A DeconstructionVickrant SinghNo ratings yet
- Overview of Cystic Fibrosis & Its ManagementDocument54 pagesOverview of Cystic Fibrosis & Its Managementvani reddyNo ratings yet
- Cystic Fibrosis Patient PamphletDocument2 pagesCystic Fibrosis Patient PamphletfloapaaNo ratings yet
- Fibrosis QuísticaDocument15 pagesFibrosis QuísticaGerardo Soto ErdelyNo ratings yet
- Running Head: Reverse Case Study 1Document15 pagesRunning Head: Reverse Case Study 1muthegetra100% (1)
- CF Respiratory Case Study Assignment (1) - 1Document4 pagesCF Respiratory Case Study Assignment (1) - 1briannaNo ratings yet
- 2022 The Changing Landscape of Nutrition in Cystic Fibrosis - The Emergence of Overweight and ObesityDocument18 pages2022 The Changing Landscape of Nutrition in Cystic Fibrosis - The Emergence of Overweight and ObesityMaria Paula CastroNo ratings yet
- 2022 Pancreatic Enzyme Replacement Therapy in Cystic FibrosisDocument11 pages2022 Pancreatic Enzyme Replacement Therapy in Cystic FibrosisMaria Paula CastroNo ratings yet
- Genetic DisordersDocument3 pagesGenetic DisordersPatricia Xandra AurelioNo ratings yet
- Nutritionalissuesin Cysticfibrosis: Missale Solomon,, Molly Bozic,, Maria R. MascarenhasDocument11 pagesNutritionalissuesin Cysticfibrosis: Missale Solomon,, Molly Bozic,, Maria R. MascarenhasDea PertiwiNo ratings yet
- 1 s2.0 S1569199323007610 MainDocument2 pages1 s2.0 S1569199323007610 MainLaura NituNo ratings yet
- 5th Edition Manual 080120Document126 pages5th Edition Manual 080120Maria TudorieNo ratings yet
- 2019 Nutrition in Cystic Fibrosis - From The Past To The Present and Into The FutureDocument18 pages2019 Nutrition in Cystic Fibrosis - From The Past To The Present and Into The FutureMaria Paula CastroNo ratings yet
- Cancer Risk in Patients With Inflammatory Bowel Disease: Materials and MethodsDocument5 pagesCancer Risk in Patients With Inflammatory Bowel Disease: Materials and MethodsVictor StefanNo ratings yet
- BIMA Oxford AZ Vaccine Detailed Position StatementDocument5 pagesBIMA Oxford AZ Vaccine Detailed Position StatementVegha NedyaNo ratings yet
- Cystic FibrosisDocument4 pagesCystic FibrosissandsphilipNo ratings yet
- American Society For Reproductive Medicine (Asrm) Patient Management and Clinical Recommendations During The Coronavirus (Covid-19) PandemicDocument8 pagesAmerican Society For Reproductive Medicine (Asrm) Patient Management and Clinical Recommendations During The Coronavirus (Covid-19) PandemicIoana Adina RugescuNo ratings yet
- COPD NationalActionPlanAug2019Document68 pagesCOPD NationalActionPlanAug2019Kristen LynchNo ratings yet
- Cystic Fibrosis PaperDocument7 pagesCystic Fibrosis Paperapi-586855789No ratings yet
- Sullivan 2015Document10 pagesSullivan 2015Andry Wahyudi AgusNo ratings yet
- Cystic FibrosisDocument3 pagesCystic FibrosisSaahil Kaura BaliNo ratings yet
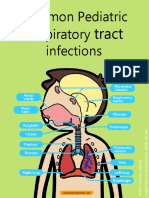
- Common Pediatric Respiratory InfectionsDocument13 pagesCommon Pediatric Respiratory InfectionsAisha JailaniNo ratings yet
- WHO-Reproductive Health Indicators-WHO 2006Document68 pagesWHO-Reproductive Health Indicators-WHO 2006revlieeNo ratings yet
- FCM Platinum ReviewerDocument24 pagesFCM Platinum ReviewerJorelle MarquezNo ratings yet
- Sas 1 60 Multiple Choice Converted CompressedDocument153 pagesSas 1 60 Multiple Choice Converted CompressedRoswell Almodiel EscaranNo ratings yet
- Fibrosis QuísticaDocument6 pagesFibrosis QuísticaKATHERINE MORALES MONTOYANo ratings yet
- The Joint Philippine Society of Gastroenterology and Philippine Society of Digestive Endoscopy Consensus Guidelines PDFDocument16 pagesThe Joint Philippine Society of Gastroenterology and Philippine Society of Digestive Endoscopy Consensus Guidelines PDFaxxoNo ratings yet
- Regular Fasting Linked To Less Severe COVID StudyDocument1 pageRegular Fasting Linked To Less Severe COVID StudylocosaltelefonoNo ratings yet
- 1 s2.0 S1526054219300235 MainDocument4 pages1 s2.0 S1526054219300235 MainBruno SantosNo ratings yet
- Undesirable Body Mass Index Profiles in Young Adults: No One Is Immune To Obesity Epidemic in PakistanDocument5 pagesUndesirable Body Mass Index Profiles in Young Adults: No One Is Immune To Obesity Epidemic in PakistanDr Alamzeb JadoonNo ratings yet
- Intravenous Albumin in Patients With Cirrhosis Evaluation of Practice Patterns and Secular Trends of Usage in Ontario 2000 To 2017Document7 pagesIntravenous Albumin in Patients With Cirrhosis Evaluation of Practice Patterns and Secular Trends of Usage in Ontario 2000 To 2017倪沁赟No ratings yet
- Cole JACI2013Document6 pagesCole JACI2013Ika KartikaNo ratings yet
- Cystic Fibrosis Ten Promising Therapeutic Approaches in The Current Era of CareDocument19 pagesCystic Fibrosis Ten Promising Therapeutic Approaches in The Current Era of CareEliana DiosaNo ratings yet
- Ppfa Annualreport 20 21 c3 DigitalDocument36 pagesPpfa Annualreport 20 21 c3 DigitalFernando MerendaNo ratings yet
- Peter Collins Nutrition Support Severe Respiratory Disease 3 Slides PPDocument19 pagesPeter Collins Nutrition Support Severe Respiratory Disease 3 Slides PPKim Nana UlfaNo ratings yet
- Cystic FibrosisDocument4 pagesCystic Fibrosisapi-548375486No ratings yet
- Cystic Fibrosis Paper FinalDocument13 pagesCystic Fibrosis Paper Finalapi-234297365No ratings yet
- CF Presentation To Stanford Family Day - March 2017Document59 pagesCF Presentation To Stanford Family Day - March 2017Tanya GreyNo ratings yet
- Bsn2 2 Cmca Lec Prelims 1Document42 pagesBsn2 2 Cmca Lec Prelims 1Joann PunzalanNo ratings yet
- Sepsis Manual 7th Edition 2024 V1.0Document112 pagesSepsis Manual 7th Edition 2024 V1.0Laras Adythia PratiwiNo ratings yet
- Pathophysiology Concepts of Altered Health States Porth 8th Edition Test BankDocument36 pagesPathophysiology Concepts of Altered Health States Porth 8th Edition Test Banksetonwedded3urss0100% (43)
- Revista InsnsbDocument112 pagesRevista InsnsbKatherine A. Adrianzén EstevesNo ratings yet
- Summer 23Document11 pagesSummer 23MUHAMMAD09No ratings yet
- FIGO HIP For Website 21 Feb 17Document46 pagesFIGO HIP For Website 21 Feb 17Bob IrsanNo ratings yet
- Cystic Fibrosis: Anita Thompson Amy Waters Matt Moore Amanda Bowes Jenn WilsonDocument28 pagesCystic Fibrosis: Anita Thompson Amy Waters Matt Moore Amanda Bowes Jenn WilsonAnita ThompsonNo ratings yet
- Factors Associated With Exclusive Breastfeeding in A Maternity Hospital Reference in Humanized Birth - PubMedDocument1 pageFactors Associated With Exclusive Breastfeeding in A Maternity Hospital Reference in Humanized Birth - PubMedVicol GrigoreNo ratings yet
- Fibroza QuizDocument5 pagesFibroza QuizBery BeryNo ratings yet
- Breastfeeding in The Philippines, A Critical Review 2013Document38 pagesBreastfeeding in The Philippines, A Critical Review 2013melabernardinoNo ratings yet
- Research Article: Hepatitis B Vaccination and Screening Awareness in Primary Care PractitionersDocument8 pagesResearch Article: Hepatitis B Vaccination and Screening Awareness in Primary Care PractitionersAnonymous xbs2ZmNo ratings yet
- Maternity and Womens Health Care 10th Edition by Lowdermilk Test BankDocument10 pagesMaternity and Womens Health Care 10th Edition by Lowdermilk Test BankDan Holland100% (29)
- Lactation: and The Risk of CancerDocument33 pagesLactation: and The Risk of CancerNeel GuptaNo ratings yet
- INFLAMMATORY Breast CancerDocument20 pagesINFLAMMATORY Breast CancerbencleeseNo ratings yet
- Senior Cycle 1 General Practice: Department of General Practice RCSI Medical School DublinDocument27 pagesSenior Cycle 1 General Practice: Department of General Practice RCSI Medical School Dublinpea_ciha05No ratings yet
- Inquiry Presentation-1Document11 pagesInquiry Presentation-1api-272568633No ratings yet
- Safety Update: COVID-19 Convalescent Plasma in 20,000 Hospitalized PatientsDocument10 pagesSafety Update: COVID-19 Convalescent Plasma in 20,000 Hospitalized PatientsVeloz RedNo ratings yet
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- Breathing Exercises: Mazyad AlotaibiDocument32 pagesBreathing Exercises: Mazyad AlotaibiekaNo ratings yet
- Patella Dislocation Association With Drop Foot: Case ReportDocument2 pagesPatella Dislocation Association With Drop Foot: Case ReportekaNo ratings yet
- Physiotherapy Management of Knee Osteoarthritis in Nigeriada Survey of Self-Reported Treatment PreferencesDocument9 pagesPhysiotherapy Management of Knee Osteoarthritis in Nigeriada Survey of Self-Reported Treatment PreferencesekaNo ratings yet
- Formulation and Product Development of Nebuliser Inhaler: An OverviewDocument6 pagesFormulation and Product Development of Nebuliser Inhaler: An OverviewekaNo ratings yet
- 5a21 PDFDocument15 pages5a21 PDFekaNo ratings yet
- 07.03.05 Breathing ExercisesDocument5 pages07.03.05 Breathing ExercisesekaNo ratings yet
- Bobath Concept Structural Framework (BCSF) : Positioning Partial Aspects Within A Holistic Therapeutic ConceptDocument7 pagesBobath Concept Structural Framework (BCSF) : Positioning Partial Aspects Within A Holistic Therapeutic ConceptekaNo ratings yet
- Jurnal Fisioterapi DadaDocument15 pagesJurnal Fisioterapi DadaekaNo ratings yet
- Nursing 20170705 01Document4 pagesNursing 20170705 01ekaNo ratings yet
- 5 Literature Review On Dizziness Based On PEDRO PDFDocument186 pages5 Literature Review On Dizziness Based On PEDRO PDFekaNo ratings yet
- Brosur & Spec - Carina System PDFDocument8 pagesBrosur & Spec - Carina System PDFHafid Sang PemimpiNo ratings yet
- Dermatitis Perioral 2015Document7 pagesDermatitis Perioral 2015Carlos Augusto Morales ChaconNo ratings yet
- Argumentative Research EssayDocument7 pagesArgumentative Research Essayajone249uncceduNo ratings yet
- Nosocomial PneumoniaDocument37 pagesNosocomial PneumoniaWinson ChitraNo ratings yet
- Nursing Diagnosis of Prostate CancerDocument3 pagesNursing Diagnosis of Prostate CancerSyafiqAzizi100% (1)
- ADA Guidelines For Infection Control 3rd EdDocument56 pagesADA Guidelines For Infection Control 3rd Edaprmaster100% (2)
- Dematologist Appointment Abhishekdixit 22oct5.20pmdigital RegistrarDocument1 pageDematologist Appointment Abhishekdixit 22oct5.20pmdigital RegistrarabhishekNo ratings yet
- Curriculum-Vitae: Ravi Shankar ChoudharyDocument3 pagesCurriculum-Vitae: Ravi Shankar ChoudharyRavi Shankar ChoudharyNo ratings yet
- FryetteDocument2 pagesFryetteSaba KhanNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS)Document3 pagesAcute Respiratory Distress Syndrome (ARDS)akish4uNo ratings yet
- Coombs TestDocument5 pagesCoombs TestMima Fatimah LuthfieNo ratings yet
- Nabh Training Topics For All The Departmental StaffDocument4 pagesNabh Training Topics For All The Departmental StaffMr. R. Ramesh75% (8)
- Cleft Lip and Cleft PalateDocument22 pagesCleft Lip and Cleft PalateOm VaishNav0% (1)
- Case Presentation: Alcoholic GastritisDocument18 pagesCase Presentation: Alcoholic Gastritisstancy thomas100% (1)
- What Is Medical Marijuana?Document8 pagesWhat Is Medical Marijuana?Dragoș TiculaNo ratings yet
- ClearPoint Healthcare KPIsDocument19 pagesClearPoint Healthcare KPIsJosue Paz100% (1)
- Ret Dem Bed Bath Hair Shampoo WUPDocument4 pagesRet Dem Bed Bath Hair Shampoo WUPCarissa De Luzuriaga-BalariaNo ratings yet
- Insomnia and Vivid Dreaming in Chinese Medical Thinking: by Heiner FruehaufDocument5 pagesInsomnia and Vivid Dreaming in Chinese Medical Thinking: by Heiner FruehaufRomi BrenerNo ratings yet
- CRM Practices in Hospitals: (Case of Fortis Hospital)Document14 pagesCRM Practices in Hospitals: (Case of Fortis Hospital)Dinesh Shende89% (9)
- Control of Blood Glucose LevelDocument21 pagesControl of Blood Glucose LevelalynnsakinaNo ratings yet
- Prevelance of Piriformis Syndrome in Chronic Low Back Pain Patients. A Clinical Diagnosis With Modified FAIR Test PainPractice20121 PDFDocument9 pagesPrevelance of Piriformis Syndrome in Chronic Low Back Pain Patients. A Clinical Diagnosis With Modified FAIR Test PainPractice20121 PDFAuliadi AnsharNo ratings yet
- Career Essay 5Document5 pagesCareer Essay 5api-490410269No ratings yet
- Perspectives On Episodic and Semantic Memory Retrieval. Chaprer 1.1 of The Book Handbook of Episodic Memory.Document2 pagesPerspectives On Episodic and Semantic Memory Retrieval. Chaprer 1.1 of The Book Handbook of Episodic Memory.Tahi GuzmánNo ratings yet
- Oxygen-Induced Hypercapnia in COPD PDFDocument4 pagesOxygen-Induced Hypercapnia in COPD PDFsatyagraha84No ratings yet
- Hydrocephalus and ADHD OverviewDocument4 pagesHydrocephalus and ADHD OverviewAlthea Ninotschka AgaloosNo ratings yet
- Issues Around Vaginal Vault Closure: ReviewDocument6 pagesIssues Around Vaginal Vault Closure: ReviewKeeranmayeeishraNo ratings yet
- Sample Nursing Examinations - Answer & Rationale-BudekDocument7 pagesSample Nursing Examinations - Answer & Rationale-BudekLj FerolinoNo ratings yet
- Pediatric PneumoniaDocument12 pagesPediatric PneumoniaKrystal Migo Denolo ContrerasNo ratings yet
- What Is Pityriasis Rosea?Document1 pageWhat Is Pityriasis Rosea?andinaNo ratings yet
- Philoderm Peeling ENG1Document60 pagesPhiloderm Peeling ENG1Niculae Bogdan Dimitrie100% (1)