You might also like
- Neurological Assessment in the First Two Years of LifeFrom EverandNeurological Assessment in the First Two Years of LifeGiovanni CioniNo ratings yet
- Clinical Observations of Motor and Postural Skills-2 Edition (COMPS-2)Document16 pagesClinical Observations of Motor and Postural Skills-2 Edition (COMPS-2)Jhon Liev100% (2)
- Therapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyFrom EverandTherapy Outcome Measures for Rehabilitation Professionals: Speech and Language Therapy, Physiotherapy, Occupational TherapyNo ratings yet
- BOTMP2Document31 pagesBOTMP2蘇永泓No ratings yet
- The Movment ABC Template For Evaluations AB-2 7-10 YearsDocument2 pagesThe Movment ABC Template For Evaluations AB-2 7-10 YearsFerris100% (1)
- Fine Motor Precision CompressDocument17 pagesFine Motor Precision CompressVictor Bravo OlivaresNo ratings yet
- OT Appendix Tables-Mar.2006Document12 pagesOT Appendix Tables-Mar.2006Yas DGNo ratings yet
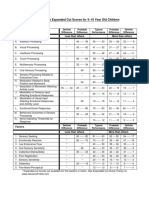
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDocument1 pageSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliNo ratings yet
- Ampsmanual Chapters1-4Document52 pagesAmpsmanual Chapters1-4Aymen DabboussiNo ratings yet
- Satco Clinical WorkbookDocument6 pagesSatco Clinical WorkbookKidz to Adultz Exhibitions100% (1)
- BOT 2 Webinar Handout 092115Document23 pagesBOT 2 Webinar Handout 092115Mikey PanupongNo ratings yet
- Activity Monitoring WorksheetDocument2 pagesActivity Monitoring WorksheetRoberto SzenczukNo ratings yet
- PeabodyDocument6 pagesPeabodyIngrid BarkoNo ratings yet
- GmfmscoresheetDocument6 pagesGmfmscoresheetapi-260049180No ratings yet
- Salhi Beery Vmi Write UpDocument4 pagesSalhi Beery Vmi Write Upapi-547482419No ratings yet
- Occupational Therapy Assessment ToolsDocument19 pagesOccupational Therapy Assessment ToolsThirdy BullerNo ratings yet
- School Function AssessmentDocument8 pagesSchool Function AssessmentPaulina Vergara67% (3)
- BRIEF - IR - Parent - Form SAMPLE PDFDocument10 pagesBRIEF - IR - Parent - Form SAMPLE PDFAna Sofía BolañosNo ratings yet
- Sipt CotaDocument2 pagesSipt CotaMónica CruzNo ratings yet
- Movement Assessment Battery For Children: 2nd Edition (MABC-2)Document20 pagesMovement Assessment Battery For Children: 2nd Edition (MABC-2)angelica barraza50% (2)
- BOT-2 Complete Form Sample Report PDFDocument12 pagesBOT-2 Complete Form Sample Report PDFmarioh_40% (1)
- MinnesotaDocument2 pagesMinnesotaOrdizia TONo ratings yet
- DTVP 2Document2 pagesDTVP 2Pradeep JNA0% (1)
- VMIpdfDocument6 pagesVMIpdfRidwan HadiputraNo ratings yet
- SPM P 3 5 Anos Home PDFDocument2 pagesSPM P 3 5 Anos Home PDFkateb dienelNo ratings yet
- M-FUN Assessment ReviewDocument4 pagesM-FUN Assessment ReviewKishan RamtohulNo ratings yet
- Ot HandbookDocument24 pagesOt Handbooktaraka sravyaNo ratings yet
- Assessments and Outcome Measures of Cerebral PalsyDocument27 pagesAssessments and Outcome Measures of Cerebral Palsyرمزي سويسيNo ratings yet
- Templete Final BOT2Document18 pagesTemplete Final BOT2Tucker OliverTriboletti50% (2)
- 1 (SPM™) Sensory Processing Measure™ - WPSDocument1 page1 (SPM™) Sensory Processing Measure™ - WPSVINEET GAIROLA0% (2)
- Sensory ProfileDocument5 pagesSensory ProfileNika GarciaNo ratings yet
- SI Theory and PracticeDocument57 pagesSI Theory and PracticeMaria Laura Soria100% (1)
- Dunn Sensory Profile InterpretationDocument5 pagesDunn Sensory Profile InterpretationScribdTranslationsNo ratings yet
- Movement ABC 2 Frequently Asked QuestionsDocument8 pagesMovement ABC 2 Frequently Asked QuestionsCat Graverobber Iskariot0% (1)
- GMFMscoresheetDocument6 pagesGMFMscoresheetAbdur RasyidNo ratings yet
- The Bayley Scales of InfantDocument10 pagesThe Bayley Scales of InfantJESUS MARTIN VILLA CARRASCONo ratings yet
- Perfil Sensorial2 0-6 MesesDocument4 pagesPerfil Sensorial2 0-6 MesesNoeliaNo ratings yet
- Pediatric Evaluation ReportDocument3 pagesPediatric Evaluation Reportapi-469965619No ratings yet
- 145 Fine Motor MilestonesDocument2 pages145 Fine Motor Milestonesapi-285528213100% (1)
- Sensory Profile 2 (SP2) : Age Range: Time To AdministerDocument3 pagesSensory Profile 2 (SP2) : Age Range: Time To Administer宗轶烜No ratings yet
- Abas ModelDocument9 pagesAbas ModelTeodora RusuNo ratings yet
- General Self-Efficacy Scale (GSE)Document2 pagesGeneral Self-Efficacy Scale (GSE)Angelus MoreNo ratings yet
- Beery Vmi Performance in Autism Spectrum DisorderDocument33 pagesBeery Vmi Performance in Autism Spectrum DisorderJayminertri Minorous100% (1)
- SPM IntroduccionDocument20 pagesSPM IntroduccionConstanzaNo ratings yet
- Pedi Cat ManualDocument163 pagesPedi Cat ManualJosh Provlin100% (1)
- 9 (SPM™) Sensory Processing Measure™ - WPSDocument1 page9 (SPM™) Sensory Processing Measure™ - WPSVINEET GAIROLANo ratings yet
- Pedi Cat Manual 1 3 6Document162 pagesPedi Cat Manual 1 3 6Cesar Cuevas100% (2)
- Otor & Visual Motor AssessDocument4 pagesOtor & Visual Motor AssessBea FloresNo ratings yet
- Assignment 7 - Artifact 3 Iep ProcessDocument10 pagesAssignment 7 - Artifact 3 Iep Processapi-549728225No ratings yet
- Caregiver Sensory ProfileDocument6 pagesCaregiver Sensory ProfileRomysah Farooq100% (1)
- Sfa Scool Function AssementDocument18 pagesSfa Scool Function AssementAnielle OliveiraNo ratings yet
- Sensory History QuestionnaireDocument6 pagesSensory History Questionnaireİpek OMUR100% (1)
- JPGN-17-205 The Pediatric Eating Assessment Tool PDFDocument7 pagesJPGN-17-205 The Pediatric Eating Assessment Tool PDFNina SalinasNo ratings yet
- BOT-2 Complete Form Sample ReportDocument12 pagesBOT-2 Complete Form Sample Reportkonna4539100% (3)
- Sensory Processing Measure (SPM) - Pearson Clinical Australia & New ZealandDocument1 pageSensory Processing Measure (SPM) - Pearson Clinical Australia & New ZealandVINEET GAIROLA0% (1)
- Ot Guidelines Child SpecificDocument34 pagesOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- EASIDocument10 pagesEASIRosario0% (1)
- GMFMDocument5 pagesGMFMc333314No ratings yet
- The Learning of Motor SkillsDocument6 pagesThe Learning of Motor SkillslyleNo ratings yet
- Unit 7 Special - Tests 7th UnitDocument71 pagesUnit 7 Special - Tests 7th UnitKaran SinghNo ratings yet
- CC BS 26 Nov 19Document48 pagesCC BS 26 Nov 19delfiaNo ratings yet
- Case Conference Monday Night Shift, March 16 2019Document42 pagesCase Conference Monday Night Shift, March 16 2019delfiaNo ratings yet
- CC 2 Oktober 2019Document54 pagesCC 2 Oktober 2019delfiaNo ratings yet
- CC BS 26 Nov 19Document48 pagesCC BS 26 Nov 19delfiaNo ratings yet
- CC 2 Oktober 2019Document54 pagesCC 2 Oktober 2019delfiaNo ratings yet
- Case Conference Saturday Night Shift, APRIL 6 TH, 2019Document46 pagesCase Conference Saturday Night Shift, APRIL 6 TH, 2019delfiaNo ratings yet
- Edrv 0513Document31 pagesEdrv 0513delfiaNo ratings yet
- Jurnal CC 19 SeptDocument12 pagesJurnal CC 19 SeptdelfiaNo ratings yet
- Approach To Reticulate Hyperpigmentation: Clinical Dermatology - Review ArticleDocument8 pagesApproach To Reticulate Hyperpigmentation: Clinical Dermatology - Review ArticledelfiaNo ratings yet
- Osmolaritas Viskositas Only For PPMDocument13 pagesOsmolaritas Viskositas Only For PPMdelfiaNo ratings yet
- CC DHF 27 Okt 2018 EditDocument68 pagesCC DHF 27 Okt 2018 EditdelfiaNo ratings yet
- CC 20 Desember 2017Document59 pagesCC 20 Desember 2017delfiaNo ratings yet
- Morning Report Thursday, 4 July 2017Document39 pagesMorning Report Thursday, 4 July 2017delfiaNo ratings yet
- Case Conference 211117 (Sepsis Neonatorum, CHD)Document61 pagesCase Conference 211117 (Sepsis Neonatorum, CHD)dhania patraNo ratings yet
- CC 31agustus 2017 KBRT Inggris EditDocument38 pagesCC 31agustus 2017 KBRT Inggris EditdelfiaNo ratings yet
- Diagnostic Study Appraisal Worksheet PDFDocument3 pagesDiagnostic Study Appraisal Worksheet PDFdian_c87No ratings yet
- CC 13 Juli 2017 MeningoencephalitisDocument40 pagesCC 13 Juli 2017 MeningoencephalitisdelfiaNo ratings yet
- CASP RCT Appraisal ToolDocument4 pagesCASP RCT Appraisal ToolNutDen R X NuttapongNo ratings yet
- CC 13 Juli 2017 MeningoencephalitisDocument40 pagesCC 13 Juli 2017 MeningoencephalitisdelfiaNo ratings yet
- SynflorixDocument45 pagesSynflorixdelfiaNo ratings yet
- Allen HDDocument2 pagesAllen HDdelfiaNo ratings yet
- UKDocument1 pageUKdelfiaNo ratings yet
- 1 s2.0 S1875957216300225 MainDocument7 pages1 s2.0 S1875957216300225 MaindelfiaNo ratings yet
- Dka CalculatorDocument1 pageDka CalculatordelfiaNo ratings yet
- Cerebellopontine Angle TumoursDocument11 pagesCerebellopontine Angle TumoursIsmail Sholeh Bahrun MakkaratteNo ratings yet
- Terapi Status EpileptikusDocument2 pagesTerapi Status EpileptikusdelfiaNo ratings yet
- CP Growth ChartDocument30 pagesCP Growth ChartJijie Azeera100% (1)
- School Psychologist ResumeDocument8 pagesSchool Psychologist Resumefvntkabdf100% (2)
- Welcome Letter and PacketDocument4 pagesWelcome Letter and PacketMuddsir Aman100% (1)
- Collaboration and Teamwork: Immersion and Presence in An Online Learning EnvironmentDocument23 pagesCollaboration and Teamwork: Immersion and Presence in An Online Learning EnvironmentLiezly DiergosNo ratings yet
- Motivating Your AudienceDocument8 pagesMotivating Your AudienceShabbirAhmadNo ratings yet
- Multiaxial Diagnosis As Per DSM IV TR in PsychiatryDocument11 pagesMultiaxial Diagnosis As Per DSM IV TR in PsychiatryVirupaksha HG100% (1)
- Leadership Through ConflictDocument8 pagesLeadership Through ConflictJ. ZhouNo ratings yet
- Peer Influence and Classroom Management Among Bse-Biology StudentsDocument52 pagesPeer Influence and Classroom Management Among Bse-Biology StudentsJenny Villa AlcantaraNo ratings yet
- Lecture - 17 Evaluation, Feedback and RewardsDocument7 pagesLecture - 17 Evaluation, Feedback and RewardsArjun MeghanathanNo ratings yet
- HW2 - PH M Thùy LinhDocument1 pageHW2 - PH M Thùy LinhThùy LinhNo ratings yet
- FILIPINO 7 - Item AnalysisDocument30 pagesFILIPINO 7 - Item AnalysisHelenLanzuelaManaloto100% (1)
- DePaul University Adult-Student Alumni RoadmapDocument2 pagesDePaul University Adult-Student Alumni RoadmapDePaul CareerCtrNo ratings yet
- Designing Learning PortfoliosDocument7 pagesDesigning Learning PortfoliosKris Mellan SabinianoNo ratings yet
- OSOT Checklist: Settling inDocument2 pagesOSOT Checklist: Settling incrimsonstained7No ratings yet
- Winning The Battle For Your Mind - Grant MullenDocument3 pagesWinning The Battle For Your Mind - Grant Mullenlisa252100% (1)
- Bob Proctor DetailsDocument3 pagesBob Proctor Detailsfpicho100% (1)
- Solucion Test 1 PDFDocument2 pagesSolucion Test 1 PDFYolanda Moya MartínezNo ratings yet
- An A From Miss Keller Part 2 2f2 - 4th GradeDocument3 pagesAn A From Miss Keller Part 2 2f2 - 4th Gradeapi-345469276No ratings yet
- Appendix Assessingcreativity PDFDocument34 pagesAppendix Assessingcreativity PDFJetmir MusaNo ratings yet
- Physiotherapists' Views, Perceived Knowledge, and Reported Use of Psychosocial Strategies in PracticeDocument16 pagesPhysiotherapists' Views, Perceived Knowledge, and Reported Use of Psychosocial Strategies in PracticeDoctor MemiNo ratings yet
- Comic-Ppt 1Document17 pagesComic-Ppt 1api-289046783No ratings yet
- Kohleerg's Theory of Moral DevelopmentDocument12 pagesKohleerg's Theory of Moral DevelopmentDavao Occidental Provincial Treasurers OfficeNo ratings yet
- Understanding and Managing RumorsDocument7 pagesUnderstanding and Managing RumorsCheung Ka WaiNo ratings yet
- Talking With Voices-Learning From The DialogueDocument3 pagesTalking With Voices-Learning From The DialogueGateway ProjectNo ratings yet
- Language and Literature Assessment (Complete)Document12 pagesLanguage and Literature Assessment (Complete)Christina Del RosarioNo ratings yet
- Compiled Course Handout - Sem 4 - SymbiosisDocument65 pagesCompiled Course Handout - Sem 4 - SymbiosisAnushka TiwaryNo ratings yet
- The Benefits of A Bilingual BrainDocument3 pagesThe Benefits of A Bilingual BrainTiên Nguyễn Thị BảoNo ratings yet
- QUESTIONNAIRE1Document2 pagesQUESTIONNAIRE1Jason AndoyoNo ratings yet
- Intelligence Test Reflection PaperDocument8 pagesIntelligence Test Reflection PaperDesiree Grace Tan-LinNo ratings yet
- Sleep Hygiene-2017Document11 pagesSleep Hygiene-2017q3rNo ratings yet
- Communication Processes, Principles, and Ethics: John Rodolf N. Mortega, Maed. Educator/WriterDocument8 pagesCommunication Processes, Principles, and Ethics: John Rodolf N. Mortega, Maed. Educator/WriterAngelica EndrenalNo ratings yet