You might also like
- Clinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenDocument4 pagesClinico-Etiological Spectrum of Pancytopenia in Hospitalized ChildrenNurul Huda KowitaNo ratings yet
- Clinical Profile and Outcome in Children of Dengue Hemorrhagic Fever in North IndiaDocument7 pagesClinical Profile and Outcome in Children of Dengue Hemorrhagic Fever in North IndiaAna Rosida SafwanNo ratings yet
- Clinical Profile and Outcome of Dengue Fever CasesDocument2 pagesClinical Profile and Outcome of Dengue Fever CasesValencius SunandarNo ratings yet
- Dengue in Pregnancy: AbstractDocument3 pagesDengue in Pregnancy: AbstractsharenNo ratings yet
- Streptococcus suis infections in ThailandDocument6 pagesStreptococcus suis infections in ThailandAram Dumnoen-ngamNo ratings yet
- Diarrhea Among Children Admitted To A Private Tertiary-Care Hospital, Bangkok, Thailand: A Case SeriesDocument9 pagesDiarrhea Among Children Admitted To A Private Tertiary-Care Hospital, Bangkok, Thailand: A Case SeriesSrkyn MeritNo ratings yet
- PARASITIC INFECTIONS IN MALAYSIADocument10 pagesPARASITIC INFECTIONS IN MALAYSIAiloveyou_143No ratings yet
- 838 3348 1 PBDocument7 pages838 3348 1 PBararapiaNo ratings yet
- Pharmaceutical Sciences: Clinical Profile and Predictors of Severe Dengue Disease: A Study From PakistanDocument5 pagesPharmaceutical Sciences: Clinical Profile and Predictors of Severe Dengue Disease: A Study From PakistaniajpsNo ratings yet
- Original ArticleDocument4 pagesOriginal ArticleGoto LaluNo ratings yet
- Resurgence of Diphtheria: Clinical Profile and Outcome - A Retrospective Observational StudyDocument4 pagesResurgence of Diphtheria: Clinical Profile and Outcome - A Retrospective Observational StudyLestari LifaNo ratings yet
- VZ 5Document5 pagesVZ 5jemia sura laksana tariganNo ratings yet
- PGH 107 04 198Document4 pagesPGH 107 04 198shjahsjanshaNo ratings yet
- Is Dengue Severity Related To Nutritional StatusDocument7 pagesIs Dengue Severity Related To Nutritional StatusrhiiryyNo ratings yet
- Pe08035 2Document7 pagesPe08035 2gythrieNo ratings yet
- A Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarDocument9 pagesA Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarLianSiahaanNo ratings yet
- Acute Rheumatic Fever Clinical Profile in Children in Western UkraineDocument5 pagesAcute Rheumatic Fever Clinical Profile in Children in Western UkraineraniaulfahNo ratings yet
- Predictors of Spontaneous Bleeding in DengueDocument4 pagesPredictors of Spontaneous Bleeding in DengueSawettachai JaitaNo ratings yet
- Our Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicDocument5 pagesOur Experience With Bicytopenia in Patients Treated at The Ankara Hospital Pediatric ClinicRonny DoankNo ratings yet
- Clinical and Laboratory Characteristics of Pediatric Dengue Fever Patients in A Tertiary Care HospitalDocument4 pagesClinical and Laboratory Characteristics of Pediatric Dengue Fever Patients in A Tertiary Care HospitalPratiwi UmbohNo ratings yet
- 5 SudharshanDocument5 pages5 SudharshaneditorijmrhsNo ratings yet
- Clinical Profile, Etiology, and Management of Hydropneumothorax: An Indian ExperienceDocument5 pagesClinical Profile, Etiology, and Management of Hydropneumothorax: An Indian ExperienceSarah DaniswaraNo ratings yet
- Kratz Bundibugyo Ebola Final3Document2 pagesKratz Bundibugyo Ebola Final3MuhammadIhsanNo ratings yet
- Sitasi 10Document6 pagesSitasi 10Putri Cyntia DewiNo ratings yet
- Bacteremia in Children-JTPDocument5 pagesBacteremia in Children-JTPRomica MarcanNo ratings yet
- Pulmonary Tuberculosis Remains an Important Complication in Nephrotic ChildrenDocument5 pagesPulmonary Tuberculosis Remains an Important Complication in Nephrotic ChildrenMaghfirah RahimaNo ratings yet
- 35 Iajps35052018-1 PDFDocument4 pages35 Iajps35052018-1 PDFiajpsNo ratings yet
- Tourniquet TestingDocument6 pagesTourniquet TestingPatrick RamosNo ratings yet
- Health20120100002 44132100Document5 pagesHealth20120100002 44132100Gautam BhallaNo ratings yet
- Pediatric Systemic Lupus Erythematosus Associated With AutoimmuneDocument9 pagesPediatric Systemic Lupus Erythematosus Associated With AutoimmunegistaluvikaNo ratings yet
- Dengue Disease Spectrum Among Infants in The 2001 Dengue Epidemic in Chennai, Tamil Nadu, IndiaDocument3 pagesDengue Disease Spectrum Among Infants in The 2001 Dengue Epidemic in Chennai, Tamil Nadu, IndiaReju VijayandranNo ratings yet
- SudaniwawiDocument7 pagesSudaniwawiMouhammed SleiayNo ratings yet
- Pancytopenia in Children: Etiological ProfileDocument4 pagesPancytopenia in Children: Etiological ProfileHanshel SatriyaNo ratings yet
- Clinical Experience of Dengue Fever in A Regional Teaching Hospital in Southern TaiwanDocument7 pagesClinical Experience of Dengue Fever in A Regional Teaching Hospital in Southern TaiwanYan Sheng HoNo ratings yet
- TrombositopeniaDocument2 pagesTrombositopeniaSoraya RezekiNo ratings yet
- Clinical Feature and Etiology of Septic Arthritis and Osteomyelitis in ChildrenDocument5 pagesClinical Feature and Etiology of Septic Arthritis and Osteomyelitis in ChildrenIfit Bagus ApriantonoNo ratings yet
- Ijmicro2020 6658445Document6 pagesIjmicro2020 6658445Anika TahsinNo ratings yet
- Acute Pyelonephritis in PregnancyDocument7 pagesAcute Pyelonephritis in PregnancyKvmLlyNo ratings yet
- Prognostic Factors and Clinical Features in Liveborn Neonates With Hydrops FetalisDocument6 pagesPrognostic Factors and Clinical Features in Liveborn Neonates With Hydrops FetalisWulan CerankNo ratings yet
- Neonatal complications of prolonged premature rupture of membranesDocument5 pagesNeonatal complications of prolonged premature rupture of membranesPaula CyntiaNo ratings yet
- Nosocomial Infections in The General Pediatric Wards of A Hospital in TurkeyDocument4 pagesNosocomial Infections in The General Pediatric Wards of A Hospital in TurkeyAmira AmouraNo ratings yet
- Diagnosis and Management of Upper Gastrointestinal Bleeding in ChildrenDocument12 pagesDiagnosis and Management of Upper Gastrointestinal Bleeding in ChildrenYoga ForeverrNo ratings yet
- Clinical Characteristics of Covid 19 Infection in The Pediatric Age Group 11019Document4 pagesClinical Characteristics of Covid 19 Infection in The Pediatric Age Group 11019Alina BabilevNo ratings yet
- Research ArticleDocument10 pagesResearch ArticlePratama Imanuel RawungNo ratings yet
- Study On Dengue Fever in Children: A Tertiary Care Hospital During Dengue Out-BreakDocument4 pagesStudy On Dengue Fever in Children: A Tertiary Care Hospital During Dengue Out-Breakblue diamondNo ratings yet
- 2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)Document6 pages2 - Adult Meningitis in A Setting of High HIV and TB Prevalence - Findings From 4961 Suspected Cases 2010 (Modelo para o Trabalho)SERGIO LOBATO FRANÇANo ratings yet
- Ajayan 2013Document3 pagesAjayan 2013Dung TranNo ratings yet
- Etiologi Efusi PleuraDocument5 pagesEtiologi Efusi Pleuratriska antonyNo ratings yet
- Medip, IJCP-2856 ODocument6 pagesMedip, IJCP-2856 OMarcelita DuwiriNo ratings yet
- Journal of SGPTDocument3 pagesJournal of SGPTEric GibsonNo ratings yet
- Adolescents With Tuberculosis-A Review of 145 Cases, 2016Document5 pagesAdolescents With Tuberculosis-A Review of 145 Cases, 2016Yoseph Arif Putra100% (1)
- Etiological Pattern and Outcome of Non-Variceal Upper G.I. BleedingDocument5 pagesEtiological Pattern and Outcome of Non-Variceal Upper G.I. BleedingJawad ZafarNo ratings yet
- Dr. Vona 12Document5 pagesDr. Vona 12Agustiawan ImronNo ratings yet
- Microbiological Evaluation of Nosocomial Infections Using NNIS SystemDocument13 pagesMicrobiological Evaluation of Nosocomial Infections Using NNIS SystemJanatinAzaNo ratings yet
- Nephrotic Syndrome Among Children in Kano: A Clinicopathological StudyDocument6 pagesNephrotic Syndrome Among Children in Kano: A Clinicopathological StudyBANGDE TVNo ratings yet
- Risk Factors For Necrotizing Enterocolitis Associated MortalityDocument7 pagesRisk Factors For Necrotizing Enterocolitis Associated MortalityvaleriaNo ratings yet
- Neutropenic Colitis in Children 2011Document4 pagesNeutropenic Colitis in Children 2011IRINA SULEY TIRADO PEREZNo ratings yet
- Fetomaternal Outcome of Pregnancy With Hepatitis E InfectionDocument4 pagesFetomaternal Outcome of Pregnancy With Hepatitis E InfectionNZ FreelancersNo ratings yet
- Original Articles: Sydenham'S ChoreaDocument4 pagesOriginal Articles: Sydenham'S ChoreaSabyasachi MukhopadhyayNo ratings yet
- Study of Heart Rate Variability in Benign Prostatic Hyperplasia - A Hospital-Based StudyDocument3 pagesStudy of Heart Rate Variability in Benign Prostatic Hyperplasia - A Hospital-Based Studydwi-148502No ratings yet
- Pharyngitis, Diagnosis and Empiric Antibiotic Treatment ConsiderationsDocument7 pagesPharyngitis, Diagnosis and Empiric Antibiotic Treatment ConsiderationsIOSRjournalNo ratings yet
- Tonsilitis - PDF Eng 2Document7 pagesTonsilitis - PDF Eng 2Ermanto D'PhytoxzNo ratings yet
- Study of Heart Rate Variability in Benign Prostatic Hyperplasia - A Hospital-Based StudyDocument3 pagesStudy of Heart Rate Variability in Benign Prostatic Hyperplasia - A Hospital-Based Studydwi-148502No ratings yet
- JournalDocument1 pageJournaldwi-148502No ratings yet
- Rhinitis PDFDocument5 pagesRhinitis PDFbrendaNo ratings yet
- Antropologi Forensik: Dr. Taufik Hidayat, M.SC, SP.FDocument46 pagesAntropologi Forensik: Dr. Taufik Hidayat, M.SC, SP.FRuslan KamilNo ratings yet
- Journal of Forensic and Legal MedicineDocument4 pagesJournal of Forensic and Legal Medicinedwi-148502No ratings yet
- Antropologi Forensik: Dr. Taufik Hidayat, M.SC, SP.FDocument46 pagesAntropologi Forensik: Dr. Taufik Hidayat, M.SC, SP.FRuslan KamilNo ratings yet
- Journal Otitis Media (THT - KL)Document6 pagesJournal Otitis Media (THT - KL)dwi-148502No ratings yet
- Journal of Forensic and Legal MedicineDocument4 pagesJournal of Forensic and Legal Medicinedwi-148502No ratings yet
- CommunityDocument10 pagesCommunitydwi-148502No ratings yet
- Jurding PDFDocument8 pagesJurding PDFCHenyLeeNo ratings yet
- Tonsilitis - PDF Eng 2Document7 pagesTonsilitis - PDF Eng 2Ermanto D'PhytoxzNo ratings yet
- Journal of Forensic and Legal MedicineDocument4 pagesJournal of Forensic and Legal Medicinedwi-148502No ratings yet
- Treating Community-Acquired PneumoniaDocument1 pageTreating Community-Acquired Pneumoniadwi-148502No ratings yet
- Jounal Siklus Anak 5 PDFDocument5 pagesJounal Siklus Anak 5 PDFdwi-148502No ratings yet
- Skripsi Obesitas Baru PDFDocument138 pagesSkripsi Obesitas Baru PDFdwi-148502No ratings yet
- Meningitis in Children Study Reveals High Case Fatality RatesDocument6 pagesMeningitis in Children Study Reveals High Case Fatality Ratesdwi-148502No ratings yet
- Investigating Diphtheria Outbreak: A Qualitative Study in Rural AreaDocument4 pagesInvestigating Diphtheria Outbreak: A Qualitative Study in Rural Areadwi-148502No ratings yet
- Bps Pendapatan Per Kapita SumbarDocument2 pagesBps Pendapatan Per Kapita Sumbardwi-148502No ratings yet
- Journal Pneumonia 1Document1 pageJournal Pneumonia 1dwi-148502No ratings yet
- Medical Orientation Exam ReviewDocument7 pagesMedical Orientation Exam ReviewSazid KhandakerNo ratings yet
- FUNGAL and PARASITIC INFECTIONSDocument3 pagesFUNGAL and PARASITIC INFECTIONSKathleen Hazel AndresNo ratings yet
- Nursing Care Plan #1Document6 pagesNursing Care Plan #1Yamete KudasaiNo ratings yet
- (ROJ-LEC) ROJoson Patient Management Process - An OverviewDocument38 pages(ROJ-LEC) ROJoson Patient Management Process - An OverviewrojosonNo ratings yet
- NCP - Impaired Gas Exchange (COPD)Document3 pagesNCP - Impaired Gas Exchange (COPD)Karen Joy ItoNo ratings yet
- Palliative Care Referral SystemDocument6 pagesPalliative Care Referral SystemNATHANIEL YERINo ratings yet
- Headache - 2001 - Jacome - Transitional Interpersonality Thunderclap HeadacheDocument4 pagesHeadache - 2001 - Jacome - Transitional Interpersonality Thunderclap HeadacheactualashNo ratings yet
- Imci ReportDocument18 pagesImci ReportRoxane AquillanNo ratings yet
- Harmening Chapter 14Document23 pagesHarmening Chapter 14I love dem Coffee (Migz)No ratings yet
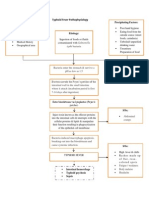
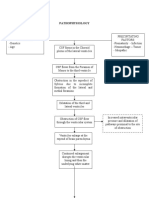
- Typhoid Fever PathophysiologyDocument1 pageTyphoid Fever Pathophysiologynesjyn75% (4)
- Jinnah Sindh Medical University: Foundation-2 Module Study Guide - MBBS Year-3, 2023 Spiral II Module TitleDocument28 pagesJinnah Sindh Medical University: Foundation-2 Module Study Guide - MBBS Year-3, 2023 Spiral II Module TitleKamlesh KumarNo ratings yet
- DISASTER Management NursingDocument68 pagesDISASTER Management Nursinglemmeloveyou01No ratings yet
- 2017 - Gastrointestinal Tract As Entry Route For Hantavirus Infection - FrontiersDocument9 pages2017 - Gastrointestinal Tract As Entry Route For Hantavirus Infection - FrontiersFlorin BranisteNo ratings yet
- AssignmentDocument5 pagesAssignmentClaire ChiuNo ratings yet
- History & Examination of Swelling, Ulcer, Sinus and FistulaDocument26 pagesHistory & Examination of Swelling, Ulcer, Sinus and Fistulaabhi_arya90% (10)
- 211 217 Libre Agua DurezaDocument7 pages211 217 Libre Agua DurezaPIERRE'S PIZZANo ratings yet
- Germ Theory: Microorganisms Cause DiseaseDocument13 pagesGerm Theory: Microorganisms Cause Diseasekinjalpatel12345No ratings yet
- Hydrocephalus PathophysiologyDocument3 pagesHydrocephalus PathophysiologyErika CadawanNo ratings yet
- Missing Microbes by Martin BlaserDocument8 pagesMissing Microbes by Martin BlasersimasNo ratings yet
- Integumentary Disorders (New)Document41 pagesIntegumentary Disorders (New)coosa liquorsNo ratings yet
- Vih GastrointestinalDocument51 pagesVih GastrointestinalRommel YánacNo ratings yet
- Dr.-andrew-moulden-EVERY VACCINE PRODUCES HARMDocument123 pagesDr.-andrew-moulden-EVERY VACCINE PRODUCES HARMPollyana Furtado Junqueira50% (4)
- 15 Patients With Altered VentilationDocument66 pages15 Patients With Altered VentilationErshelle Mae MorlaNo ratings yet
- Chap2 Lesson 1-4Document43 pagesChap2 Lesson 1-4Renalf Ezra BarbietoNo ratings yet
- Diagnosis and Management of Hyperglycemic Emergencies: Hormones (Athens, Greece) October 2011Document12 pagesDiagnosis and Management of Hyperglycemic Emergencies: Hormones (Athens, Greece) October 2011nia rahayu wNo ratings yet
- Hand Hygiene GuideDocument151 pagesHand Hygiene GuideEmmanuel CuevasNo ratings yet
- Infective EndocarditisDocument18 pagesInfective EndocarditisLee Foo WengNo ratings yet
- Medication Guide: LATUDA (luh-TOO-duh) (Lurasidone Hydrochloride) TabletsDocument2 pagesMedication Guide: LATUDA (luh-TOO-duh) (Lurasidone Hydrochloride) TabletsAmin AhmedNo ratings yet
- Risk Factors For Cutaneous Adverse Drug ReactionsDocument26 pagesRisk Factors For Cutaneous Adverse Drug ReactionsMukesh Kumar SharmaNo ratings yet
- Medik FamiliDocument10 pagesMedik FamiliBig DaddyCoolNo ratings yet