You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Gynecology Reconstructive Surgery - Volume 2Document318 pagesGynecology Reconstructive Surgery - Volume 2Bharti Pant GahtoriNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Suture MaterialDocument7 pagesSuture Materialtaner_soysuren100% (1)
- MatsumotoDocument4 pagesMatsumotodeemoney3100% (1)
- A Checklist To Improve Patient Safety in Interventional RadiologyDocument8 pagesA Checklist To Improve Patient Safety in Interventional Radiologyaegysabetterway100% (1)
- 2011 Surgery IIDocument67 pages2011 Surgery IIamruthkiranbabuji100% (1)
- Cardiac MRI Made Easy 2008Document164 pagesCardiac MRI Made Easy 2008Benjamin Gonzalez100% (1)
- Treatment of Endodontic EmergenciesDocument7 pagesTreatment of Endodontic EmergenciescemoaraNo ratings yet
- Nursing Care of Clients With Altered PerceptionDocument83 pagesNursing Care of Clients With Altered PerceptionDanica Franco100% (1)
- 2020 - 10 - 29 - Εγκεφαλικά Ημισφαίρια και Αγγειακά Σύνδρομα - ΜήτσιαςDocument67 pages2020 - 10 - 29 - Εγκεφαλικά Ημισφαίρια και Αγγειακά Σύνδρομα - ΜήτσιαςΖέτα ΤσίρκαNo ratings yet
- Forcep Delivery LPDocument7 pagesForcep Delivery LPSandhya Gupta100% (1)
- Guidelines by An Ad Hoc European Committee On Adequacy of The Paediatric Peritoneal Dialysis PrescriptionDocument6 pagesGuidelines by An Ad Hoc European Committee On Adequacy of The Paediatric Peritoneal Dialysis PrescriptionEvelina Navi BraginskiyNo ratings yet
- DapusDocument5 pagesDapusEvelina Navi BraginskiyNo ratings yet
- Chronic Kidney Disease in ChildrenDocument8 pagesChronic Kidney Disease in ChildrenEvelina Navi BraginskiyNo ratings yet
- Hemodialysis: Diffusion and Ultrafiltration: Ramin SamDocument17 pagesHemodialysis: Diffusion and Ultrafiltration: Ramin SamEvelina Navi BraginskiyNo ratings yet
- Handbook of Dialysis, Fourth Edition: John T. Daugirdas, MD Peter Blake, MD and Todd S. Ing, MDDocument1 pageHandbook of Dialysis, Fourth Edition: John T. Daugirdas, MD Peter Blake, MD and Todd S. Ing, MDEvelina Navi BraginskiyNo ratings yet
- A Literature Based Comparison of Bone Augmentation.1Document6 pagesA Literature Based Comparison of Bone Augmentation.1drzana78No ratings yet
- CV MikhailDocument2 pagesCV MikhailMikhail NurhariNo ratings yet
- Case RatesDocument306 pagesCase RatesCyril DaguilNo ratings yet
- Rozina Ali - Mail On Sunday 17 May 2015Document1 pageRozina Ali - Mail On Sunday 17 May 2015Rozina Ali PlasticSurgeryNo ratings yet
- Acute Arterial Occlusion of The Lower ExtremitiesDocument10 pagesAcute Arterial Occlusion of The Lower ExtremitiesLinda SugiartoNo ratings yet
- اسئله جراحه مدققهDocument59 pagesاسئله جراحه مدققهNour AhmededNo ratings yet
- 4 RehabilitationmanagementDocument20 pages4 RehabilitationmanagementRabia SaeedNo ratings yet
- Lecturio 3663 JaundiceDocument12 pagesLecturio 3663 JaundicePranjali WeladiNo ratings yet
- Uganda Charitable Spine Surgery Mission 2013 Trip Report Ver 1 Sept 15Document29 pagesUganda Charitable Spine Surgery Mission 2013 Trip Report Ver 1 Sept 15api-197209808No ratings yet
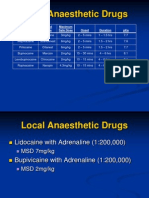
- Local Anaesthetic Drugs 3 Power Point PresentationDocument30 pagesLocal Anaesthetic Drugs 3 Power Point PresentationJosef Cefai100% (1)
- Epidermal Skin GraftingDocument5 pagesEpidermal Skin GraftingGiovanna OsornoNo ratings yet
- Advanced Cardiovascular Life Support (Acls)Document45 pagesAdvanced Cardiovascular Life Support (Acls)Erinne DefrianiNo ratings yet
- 婦兒combine 15678850 洪紫婕之子 Tracheal Stenosis, Air-leak Syndrome, Imperforate Anus, Duodenal AtresiaDocument35 pages婦兒combine 15678850 洪紫婕之子 Tracheal Stenosis, Air-leak Syndrome, Imperforate Anus, Duodenal Atresia鄧沛元醫師No ratings yet
- Stok Benang Kamar OperasiDocument5 pagesStok Benang Kamar OperasirendyNo ratings yet
- Test Bank Adult Health Nursing 7th Edition Cooper GosnellDocument15 pagesTest Bank Adult Health Nursing 7th Edition Cooper GosnellCarolina Chapman100% (31)
- Cardio. Vascular System (The Circulatory System) : Blood 2' HeartDocument12 pagesCardio. Vascular System (The Circulatory System) : Blood 2' Heartعزوز الراويNo ratings yet
- Internal Anatomy of SCDocument11 pagesInternal Anatomy of SCRuth AlbaricoNo ratings yet
- Mast Cell - Source - PosterDocument1 pageMast Cell - Source - PosterNolberto JaramilloNo ratings yet
- Prof. Dr. Hamdi Karakayalı CVDocument3 pagesProf. Dr. Hamdi Karakayalı CVyousra charaouiNo ratings yet
- June 2020 DNB Question BankDocument3 pagesJune 2020 DNB Question Bankvittal iNo ratings yet