You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Basic Arrhythmia RulesDocument3 pagesBasic Arrhythmia Rulesgreenflames0997% (30)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cardiac ArrhythmiasDocument60 pagesCardiac ArrhythmiasMelissa Monique Peart-YatesNo ratings yet
- Basic EKG Interpretation ExamDocument13 pagesBasic EKG Interpretation Examtwdroppoint100% (1)
- Basic Ecg: A Report By: Clinical Clerk Mary Hazel TeDocument74 pagesBasic Ecg: A Report By: Clinical Clerk Mary Hazel TeHazel Arcosa100% (1)
- ECG QuizDocument6 pagesECG QuizIsland Rae100% (1)
- ACLS AlgorithmsDocument4 pagesACLS Algorithmsmonickams100% (1)
- Ecg 111029102429 Phpapp01Document103 pagesEcg 111029102429 Phpapp01Vickry WahidjiNo ratings yet
- Dr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFDocument7 pagesDr. Smith's ECG Blog - "Shark Fin" - A Deadly ECG Sign That You Must Know! PDFZACHARIAH MANKIRNo ratings yet
- ACLS Review TestDocument5 pagesACLS Review Testtostc60% (5)
- Desfibrilador DEA LifepointDocument22 pagesDesfibrilador DEA LifepointabeklNo ratings yet
- Ezra Nehemiah RulebookDocument40 pagesEzra Nehemiah RulebookChalikias GeorgeNo ratings yet
- Abscess With Bioprosthetic ValveDocument2 pagesAbscess With Bioprosthetic ValveChalikias GeorgeNo ratings yet
- Carotid Sinus MassageDocument4 pagesCarotid Sinus MassageChalikias GeorgeNo ratings yet
- Consensus Antithrombotic Therapy in AF in Patients With Acute Coronary Syndrome and Undergoing Percutaneous Coronary or Valve InterventionsDocument25 pagesConsensus Antithrombotic Therapy in AF in Patients With Acute Coronary Syndrome and Undergoing Percutaneous Coronary or Valve InterventionsChalikias GeorgeNo ratings yet
- Atherosclerosis 2007Document8 pagesAtherosclerosis 2007Chalikias GeorgeNo ratings yet
- Guidelines For The Echocardiographic Assessment ofDocument29 pagesGuidelines For The Echocardiographic Assessment ofospinu6780No ratings yet
- Fluke Biomedical Product Catalogue 1 CompressedDocument24 pagesFluke Biomedical Product Catalogue 1 CompressedVini H.S.L de AlmeidaNo ratings yet
- Qrs Complexes: Fast & Easy Ecgs - A Self-Paced Learning ProgramDocument49 pagesQrs Complexes: Fast & Easy Ecgs - A Self-Paced Learning ProgramMuhammad Hatta HamzahNo ratings yet
- The HeartDocument58 pagesThe HeartJULIUS NAKANYALANo ratings yet
- BCS EkgDocument55 pagesBCS Ekggita suariyaniNo ratings yet
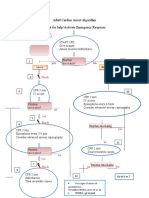
- Adult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseDocument1 pageAdult Cardiac Arrest Algorithm Shout For Help/activate Emergency ResponseICU RSBMNo ratings yet
- 2.500548 Medilog Holter System PP en LQDocument8 pages2.500548 Medilog Holter System PP en LQIvan CvasniucNo ratings yet
- Lab 2jhghgdfgxzDocument47 pagesLab 2jhghgdfgxzanaNo ratings yet
- FREE 2021 ACLS Study Guide - ACLS Made Easy!Document32 pagesFREE 2021 ACLS Study Guide - ACLS Made Easy!Alen ArguellesNo ratings yet
- EKG Interpretation Exercise: Dr. Thomas Adhi Nugroho Chaidir RSRT - Tim IcuDocument29 pagesEKG Interpretation Exercise: Dr. Thomas Adhi Nugroho Chaidir RSRT - Tim IcuThomasAdhiNugrohoChaidirNo ratings yet
- 4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - SurgeryDocument60 pages4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - Surgeryqobsar100% (1)
- Common Ecg Abnormalities PDFDocument2 pagesCommon Ecg Abnormalities PDFRonNo ratings yet
- CLC SyndromeDocument17 pagesCLC SyndromeOlga GoryachevaNo ratings yet
- European Journal of Internal MedicineDocument4 pagesEuropean Journal of Internal Medicinesamer battatNo ratings yet
- Siemens Acuson Sc2000 Ep Flyer v2Document4 pagesSiemens Acuson Sc2000 Ep Flyer v2bashir019No ratings yet
- Simplified ACLS AlgorithmDocument1 pageSimplified ACLS AlgorithmBrianNo ratings yet
- Lesson 5 ECG BiopacDocument6 pagesLesson 5 ECG BiopacJavier VeintimillaNo ratings yet
- Electrocardiographic Interpretation of Cardiac Muscle and Coronary Blood FlowDocument1 pageElectrocardiographic Interpretation of Cardiac Muscle and Coronary Blood FlowmcwnotesNo ratings yet
- Left Bundle Branch Block - UpToDateDocument25 pagesLeft Bundle Branch Block - UpToDateKrull TTTeamNo ratings yet
- ECG NotesDocument8 pagesECG NotesPeer TutorNo ratings yet
- Cardiofax Ecg 9020k ManualDocument36 pagesCardiofax Ecg 9020k ManualViviana Páez RojasNo ratings yet