You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Deadly Deception - Robert WillnerDocument303 pagesDeadly Deception - Robert Willnerleocarvalho001_60197100% (5)
- CardiologyDocument52 pagesCardiologyDexzal100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Mood Disorders - Psychology ProjectDocument16 pagesMood Disorders - Psychology ProjectKanika Mathew100% (1)
- MBF90324234Document407 pagesMBF90324234Emad Mergan100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Criminal SociologyDocument53 pagesCriminal SociologyJackielyn cabayaoNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Adult BLSDocument22 pagesAdult BLSnessaoliveiraNo ratings yet
- Canadian Pharmacy Review Ver1Document6 pagesCanadian Pharmacy Review Ver1Dr-Usman Khan30% (10)
- 100 Questions in Cardiology-, PDFDocument241 pages100 Questions in Cardiology-, PDFditairinaNo ratings yet
- Abnormal Psychology Final Practice QuestionsDocument16 pagesAbnormal Psychology Final Practice QuestionsJames WilkesNo ratings yet
- 2015 JC2 GP H1 Prelim PapersDocument357 pages2015 JC2 GP H1 Prelim PapersofficialJCUOLnotes100% (6)
- BTS Sarcoidosis Clinical StatementDocument17 pagesBTS Sarcoidosis Clinical StatementDarrin WiebeNo ratings yet
- IntroductionDocument1 pageIntroductionDexzalNo ratings yet
- Sudden Cardiac ArrestDocument2 pagesSudden Cardiac ArrestDexzalNo ratings yet
- Out of Hospital Cardiac ArrestDocument3 pagesOut of Hospital Cardiac ArrestDexzalNo ratings yet
- hASIL tPADocument2 pageshASIL tPADexzalNo ratings yet
- Advanced Cardiac Life Support PDFDocument9 pagesAdvanced Cardiac Life Support PDFYulias YoweiNo ratings yet
- Hello.. My Name Is Rizal.Document1 pageHello.. My Name Is Rizal.DexzalNo ratings yet
- Follow Up Pasien PscbaDocument10 pagesFollow Up Pasien PscbaDexzalNo ratings yet
- Can Megaloblastic Anemia Mask Thrombocytosisin Essential ThrombocytemiaDocument2 pagesCan Megaloblastic Anemia Mask Thrombocytosisin Essential ThrombocytemiaDexzalNo ratings yet
- Intensive Care Nursery House Staff ManualDocument3 pagesIntensive Care Nursery House Staff ManualgalaxytwyNo ratings yet
- Can Megaloblastic Anemia Mask Thrombocytosisin Essential Thrombocytemia PDFDocument2 pagesCan Megaloblastic Anemia Mask Thrombocytosisin Essential Thrombocytemia PDFDexzalNo ratings yet
- PDCI Core Kit 15 Early Detection and Prevention of Diabetic FootDocument22 pagesPDCI Core Kit 15 Early Detection and Prevention of Diabetic FootDexzalNo ratings yet
- PDCI Core Kit 15 Early Detection and Prevention of Diabetic Foot Dr. Hendra ZufryDocument46 pagesPDCI Core Kit 15 Early Detection and Prevention of Diabetic Foot Dr. Hendra ZufryDexzal100% (1)
- Cortical Swallowing Processing in Early Subacute Stroke PDFDocument14 pagesCortical Swallowing Processing in Early Subacute Stroke PDFDexzalNo ratings yet
- Ecg Diagnostic ToolsDocument42 pagesEcg Diagnostic ToolsDexzal100% (1)
- PDCI Core Kit 12 Insulin Injection TechniqueDocument12 pagesPDCI Core Kit 12 Insulin Injection TechniqueDexzalNo ratings yet
- Drug Resistance of TBDocument17 pagesDrug Resistance of TBGaurav Sharma100% (1)
- Arrythmia (Rev)Document53 pagesArrythmia (Rev)DexzalNo ratings yet
- PDCI Core Kit 12 Insulin Injection Technique Dr. Hendra ZufriDocument25 pagesPDCI Core Kit 12 Insulin Injection Technique Dr. Hendra ZufriDexzalNo ratings yet
- Jurnal Simposium Nasional Asma IdaiDocument29 pagesJurnal Simposium Nasional Asma IdaiRefangga Lova Efendi100% (2)
- Prevalensi ESBL PDFDocument8 pagesPrevalensi ESBL PDFDexzal100% (1)
- Dinding Thorax: DR - Rosaria IndahDocument102 pagesDinding Thorax: DR - Rosaria IndahEgaSuharnoNo ratings yet
- Guideline Management CHFDocument35 pagesGuideline Management CHFDexzalNo ratings yet
- Inborn Error of MetabolismDocument6 pagesInborn Error of MetabolismDexzalNo ratings yet
- 12 Leads EcgDocument45 pages12 Leads EcgDexzalNo ratings yet
- Music Therapy in Nursing HomesDocument7 pagesMusic Therapy in Nursing Homesapi-300510538No ratings yet
- STS Activity-18 Research-ActivityDocument2 pagesSTS Activity-18 Research-ActivityEvan Caringal SabioNo ratings yet
- Acid Base PhysiologyDocument1 pageAcid Base PhysiologyHAMMYER ALROKHAMINo ratings yet
- Virtual Care: Advancing The Practice of Veterinary Medicine: Advances in Small Animal Medicine and Surgery April 2019Document4 pagesVirtual Care: Advancing The Practice of Veterinary Medicine: Advances in Small Animal Medicine and Surgery April 2019Anonymous TDI8qdYNo ratings yet
- ENGLISH 6 - Q4 - Wk7 - USLeM RTPDocument11 pagesENGLISH 6 - Q4 - Wk7 - USLeM RTPtrishajilliene nacisNo ratings yet
- The Effects of The Concept of Minimalism On Today S Architecture Expectations After Covid 19 PandemicDocument19 pagesThe Effects of The Concept of Minimalism On Today S Architecture Expectations After Covid 19 PandemicYena ParkNo ratings yet
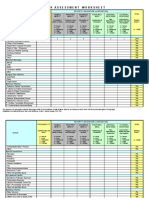
- IC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Document4 pagesIC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Juon Vairzya AnggraeniNo ratings yet
- Aluminum in Co Ffee: AccessDocument9 pagesAluminum in Co Ffee: AccessJohnNo ratings yet
- ResearchDocument28 pagesResearchReylon PachesNo ratings yet
- Classifying Giant Cell Lesions A Review.21Document5 pagesClassifying Giant Cell Lesions A Review.21shehla khanNo ratings yet
- Fertilization Reflection PaperDocument2 pagesFertilization Reflection PaperCrisandro Allen Lazo100% (2)
- Resveratrol and Its Effects On Human Health and LongevityDocument367 pagesResveratrol and Its Effects On Human Health and LongevityArnulfo Yu LanibaNo ratings yet
- Nail Disorder and DiseasesDocument33 pagesNail Disorder and Diseasesleny90941No ratings yet
- Dula-Tungkulin o Gampanin NG ProduksyonDocument12 pagesDula-Tungkulin o Gampanin NG ProduksyonBernadette DuranNo ratings yet
- DOPR Vision 2030Document36 pagesDOPR Vision 2030Hendi HendriansyahNo ratings yet
- Arthur CrawfordDocument308 pagesArthur CrawfordRupali Mokashi100% (1)
- 3E - Agustin, Anne Julia - Group 1 - Case 7,8Document5 pages3E - Agustin, Anne Julia - Group 1 - Case 7,8Anne Julia AgustinNo ratings yet
- GIEEE TGMP Policy Terms For 2022-23Document5 pagesGIEEE TGMP Policy Terms For 2022-23Janardhan Reddy TNo ratings yet
- Malawi Clinical HIV Guidelines 2019 Addendumversion 8.1Document28 pagesMalawi Clinical HIV Guidelines 2019 Addendumversion 8.1INNOCENT KHULIWANo ratings yet
- CATHETERIZATIONDocument3 pagesCATHETERIZATIONrnrmmanphdNo ratings yet
- LAN Party Skate Park by Shane Jesse ChristmassDocument91 pagesLAN Party Skate Park by Shane Jesse ChristmassPatrick TrottiNo ratings yet
- Histopathology of Dental CariesDocument7 pagesHistopathology of Dental CariesJOHN HAROLD CABRADILLANo ratings yet