You might also like
- Barriers To Pursing A Career in Surgery Alexandra MDocument7 pagesBarriers To Pursing A Career in Surgery Alexandra MSusan FernándezNo ratings yet
- Career and Professional Satisfaction of Oral and Maxillofacial Surgery Residents, Academic Surgeons, and Private Practitioners: Does Gender Matter?Document12 pagesCareer and Professional Satisfaction of Oral and Maxillofacial Surgery Residents, Academic Surgeons, and Private Practitioners: Does Gender Matter?temesgenNo ratings yet
- Patient Preference For Physician Gender in The Emergency DepartmentDocument12 pagesPatient Preference For Physician Gender in The Emergency DepartmentLuciaNo ratings yet
- Female Vs Male Surgeons: Better Outcomes?: Journal Article - Operating RoomDocument6 pagesFemale Vs Male Surgeons: Better Outcomes?: Journal Article - Operating RoomRaidis PangilinanNo ratings yet
- J Jss 2017 05 075Document9 pagesJ Jss 2017 05 075NIWAYANRADHANo ratings yet
- Endocr 4Document16 pagesEndocr 4Bogdan GavrilNo ratings yet
- Gender Comparisons of Medical Students' Psychosocial Pro®lesDocument8 pagesGender Comparisons of Medical Students' Psychosocial Pro®lesRosyiidta JanahNo ratings yet
- Endocr 1Document7 pagesEndocr 1Bogdan GavrilNo ratings yet
- Barriers To Careers Identified by Women in Academic Surgery CochranDocument6 pagesBarriers To Careers Identified by Women in Academic Surgery CochranSusan FernándezNo ratings yet
- ANZ Journal of Surgery - 2022 - Meyer - Women S Interest in Surgery As A Career in The Early Postgraduate Period ADocument7 pagesANZ Journal of Surgery - 2022 - Meyer - Women S Interest in Surgery As A Career in The Early Postgraduate Period ASusan FernándezNo ratings yet
- Impact of Gender Bias On Male Nursing Students Competence of SkillsDocument13 pagesImpact of Gender Bias On Male Nursing Students Competence of Skillsapi-526815418No ratings yet
- Comparison of Hospital Mortality and Readmission Rates For Medicare Patients Treated by Male Vs Female PhysiciansDocument8 pagesComparison of Hospital Mortality and Readmission Rates For Medicare Patients Treated by Male Vs Female PhysiciansDAVID CAMILO GOMEZ MEDINANo ratings yet
- The Impact of Role Models On Medical Students: Scott Wright, MD, Annie Wong, MD, Carol Newill, MD, PHDDocument4 pagesThe Impact of Role Models On Medical Students: Scott Wright, MD, Annie Wong, MD, Carol Newill, MD, PHDAndrea SuarezNo ratings yet
- The Impact of Gender On High-Stakes Dental EvaluationsDocument7 pagesThe Impact of Gender On High-Stakes Dental EvaluationsVijaya ChandraNo ratings yet
- Gender Based Microaggressions in Surgery A Scoping ReviewDocument14 pagesGender Based Microaggressions in Surgery A Scoping ReviewSusan FernándezNo ratings yet
- International Journal of Nursing Sciences: ReviewDocument12 pagesInternational Journal of Nursing Sciences: ReviewChristin LapadjiNo ratings yet
- Self-assessment Questions for Clinical Molecular GeneticsFrom EverandSelf-assessment Questions for Clinical Molecular GeneticsRating: 5 out of 5 stars5/5 (1)
- Groomind DoctorsDocument8 pagesGroomind DoctorsupalanisamyNo ratings yet
- Can I Cut It? Medical Students' Perceptions of Surgeons and Surgical CareersDocument8 pagesCan I Cut It? Medical Students' Perceptions of Surgeons and Surgical Careersakmal shahzadNo ratings yet
- How Sex and Gender Impact Clinical Practice: An Evidence-Based Guide to Patient CareFrom EverandHow Sex and Gender Impact Clinical Practice: An Evidence-Based Guide to Patient CareMarjorie R. JenkinsNo ratings yet
- Penelitian Cross-Sectional 3 PDFDocument29 pagesPenelitian Cross-Sectional 3 PDFSherin AlindaNo ratings yet
- Diagnostic Problems in Tumors of Head and Neck: Selected TopicsFrom EverandDiagnostic Problems in Tumors of Head and Neck: Selected TopicsRating: 5 out of 5 stars5/5 (1)
- Jamasurgery Schlick 2021 Oi 210049 1633626634.81152Document11 pagesJamasurgery Schlick 2021 Oi 210049 1633626634.81152sesa islianaNo ratings yet
- Nurse Education in Practice: Nianqi Cui, Ruoxi Wang, Feng Song, Jingfen JinDocument6 pagesNurse Education in Practice: Nianqi Cui, Ruoxi Wang, Feng Song, Jingfen JinBIETRIS WARISYUNo ratings yet
- Clinical Practice Guidelines For Antimicrobial Prophylaxis in Surgery (Update 2013)Document89 pagesClinical Practice Guidelines For Antimicrobial Prophylaxis in Surgery (Update 2013)เด็กชายสมันตภัทร แฟนคลับอาจารย์กวงNo ratings yet
- Dilemmas in ERCP: A Clinical CasebookFrom EverandDilemmas in ERCP: A Clinical CasebookDaniel K. MulladyNo ratings yet
- Articulo OftalmologiaDocument8 pagesArticulo Oftalmologiafn_millardNo ratings yet
- Concise Epidemiologic Principles and Concepts: Guidelines for Clinicians and Biomedical ResearchersFrom EverandConcise Epidemiologic Principles and Concepts: Guidelines for Clinicians and Biomedical ResearchersNo ratings yet
- Hospital Nurse Staffing PDFDocument7 pagesHospital Nurse Staffing PDFmku 2017No ratings yet
- Hair Transplant Surgery and Platelet Rich Plasma: Evidence-Based EssentialsFrom EverandHair Transplant Surgery and Platelet Rich Plasma: Evidence-Based EssentialsLinda N. LeeNo ratings yet
- Endocr 3Document10 pagesEndocr 3Bogdan GavrilNo ratings yet
- Integrating Pathology and Radiology Disciplines: An Emerging Opportunity?Document7 pagesIntegrating Pathology and Radiology Disciplines: An Emerging Opportunity?Peko PekoNo ratings yet
- Predictors of Research Utilization Among Jordanian Registered Nurses: A Descriptive Correlational StudyDocument9 pagesPredictors of Research Utilization Among Jordanian Registered Nurses: A Descriptive Correlational Studysumaia abuhatabNo ratings yet
- Family Physicians' Experiences of Physical Examination: Martina Ann Kelly, Lisa Kathryn Freeman, Tim DornanDocument7 pagesFamily Physicians' Experiences of Physical Examination: Martina Ann Kelly, Lisa Kathryn Freeman, Tim DornanMahmoud AbouelsoudNo ratings yet
- Interprofesional EducationDocument8 pagesInterprofesional EducationMirela AlexandruNo ratings yet
- Family-Focused Nursing Care of Hospitalized Elderly: Jo Ann H. Collier, PH.D., R.NDocument9 pagesFamily-Focused Nursing Care of Hospitalized Elderly: Jo Ann H. Collier, PH.D., R.NLyndon SayongNo ratings yet
- Xepoleas2020 Article TheExperiencesOfFemaleSurgeonsDocument28 pagesXepoleas2020 Article TheExperiencesOfFemaleSurgeonsOpeyemi OyeyemiNo ratings yet
- Interruptions Then and Now - Impact On Nurses' Clinical Reasoning, Emotions, and Medication SafetyDocument7 pagesInterruptions Then and Now - Impact On Nurses' Clinical Reasoning, Emotions, and Medication SafetyCONSTANZANo ratings yet
- Bourne 1978Document11 pagesBourne 1978Néstor ParedesNo ratings yet
- 10.1515 - Jom 1991 900816Document30 pages10.1515 - Jom 1991 900816Goce AndonoskiNo ratings yet
- Coetzee2013 PDFDocument12 pagesCoetzee2013 PDFfaria ejazNo ratings yet
- Review of Related LiteratureDocument6 pagesReview of Related LiteratureSOPHIA ALESNANo ratings yet
- Bmjopen 2014 006578Document18 pagesBmjopen 2014 006578Ortopedia HGMNo ratings yet
- Team Communication: It's About Patient Safety: by Susan B. Childress, RN, MN, OCNDocument4 pagesTeam Communication: It's About Patient Safety: by Susan B. Childress, RN, MN, OCNAnna Zhifa AbNo ratings yet
- Comprehensive Healthcare Simulation: Mastery Learning in Health Professions EducationFrom EverandComprehensive Healthcare Simulation: Mastery Learning in Health Professions EducationNo ratings yet
- The Grade Debate Evidence, Knowledge Gaps, and PeDocument5 pagesThe Grade Debate Evidence, Knowledge Gaps, and PeEmilio AssisNo ratings yet
- Genetics/Genomics Nursing: Scope and Standards of PracticeFrom EverandGenetics/Genomics Nursing: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (1)
- Interprofessional Teamwork Skills As Predictors of Clinical Outcomes in A Simulated Healthcare SettingDocument6 pagesInterprofessional Teamwork Skills As Predictors of Clinical Outcomes in A Simulated Healthcare SettingNavis NaldoNo ratings yet
- Complex Regional Pain Syndrome - What is the Evidence?: Ebook FormatFrom EverandComplex Regional Pain Syndrome - What is the Evidence?: Ebook FormatNo ratings yet
- Sessionsetal High Alert Meds 919 JANDocument15 pagesSessionsetal High Alert Meds 919 JANichabojanNo ratings yet
- Sex Difference in Career Aspiration of Physical TherapistDocument13 pagesSex Difference in Career Aspiration of Physical TherapistRamsha NawabNo ratings yet
- A Narrative Review of The Impact of Work Hours and Insufficient Rest On JobDocument15 pagesA Narrative Review of The Impact of Work Hours and Insufficient Rest On JobTiti DarabanNo ratings yet
- Bedside Teaching of Medical StudentsDocument2 pagesBedside Teaching of Medical StudentsRafi Ullah HaleemNo ratings yet
- Mentorship in An Academic Medical CenterDocument4 pagesMentorship in An Academic Medical CenternoniinnNo ratings yet
- PROLOG: Patient Management in OfficeFrom EverandPROLOG: Patient Management in OfficeRating: 5 out of 5 stars5/5 (4)
- 420 Research PaperDocument12 pages420 Research Paperapi-372913673No ratings yet
- Emery and Rimoin’s Principles and Practice of Medical Genetics and Genomics: Clinical Principles and ApplicationsFrom EverandEmery and Rimoin’s Principles and Practice of Medical Genetics and Genomics: Clinical Principles and ApplicationsReed E. PyeritzNo ratings yet
- Agotamiento en Personal Quirurgico Curr Prob Surg Sept 2017Document50 pagesAgotamiento en Personal Quirurgico Curr Prob Surg Sept 2017Luis ParraNo ratings yet
- The Double-Edged Scalpel: Experiences and Perceptions of Pregnancy and Parenthood During Canadian Surgical Residency TrainingDocument11 pagesThe Double-Edged Scalpel: Experiences and Perceptions of Pregnancy and Parenthood During Canadian Surgical Residency TrainingNikhil ChoudharyNo ratings yet
- Literature Review Medication Safety in Acute Care in AustraliaDocument8 pagesLiterature Review Medication Safety in Acute Care in AustraliaafdtytirdNo ratings yet
- Obstetric Hemorrhage AnestDocument9 pagesObstetric Hemorrhage AnestjefeNo ratings yet
- Lactate FaqDocument4 pagesLactate FaqMuhammad RizqiNo ratings yet
- Modifying Ventilator Settings Based On The PaCO2Document1 pageModifying Ventilator Settings Based On The PaCO2Dipesh ShresthaNo ratings yet
- Management of Obstetric Haemorrhage 3 1Document8 pagesManagement of Obstetric Haemorrhage 3 1Dipesh Shrestha100% (1)
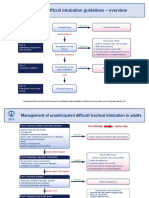
- DAS Difficult Intubation Guidelines - Overview: Plan ADocument3 pagesDAS Difficult Intubation Guidelines - Overview: Plan AMaufer AlNo ratings yet
- Common Sense On Mutual Funds 2Document1 pageCommon Sense On Mutual Funds 2Dipesh ShresthaNo ratings yet
- Moles, Osmoles, and Movement - Fact Sheet - 0Document7 pagesMoles, Osmoles, and Movement - Fact Sheet - 0Dipesh ShresthaNo ratings yet
- BPKIHSDocument38 pagesBPKIHSDipesh ShresthaNo ratings yet
- Clincal Sciences Major R..Document6 pagesClincal Sciences Major R..Dipesh ShresthaNo ratings yet
- CHS MCQ Self AssessmentDocument7 pagesCHS MCQ Self AssessmentDipesh ShresthaNo ratings yet
- The What and Why of Mechanical VentilationDocument1 pageThe What and Why of Mechanical VentilationDipesh ShresthaNo ratings yet
- Clinical Sciences Medicine Self AssessmentDocument6 pagesClinical Sciences Medicine Self AssessmentDipesh ShresthaNo ratings yet
- IBE II MCQ Questions 4th BatchDocument18 pagesIBE II MCQ Questions 4th BatchDipesh ShresthaNo ratings yet
- SJT 1Document64 pagesSJT 1Dipesh ShresthaNo ratings yet
- Surgical Safety ChecklistDocument1 pageSurgical Safety Checklistmillechilli1No ratings yet
- SJT 2Document64 pagesSJT 2Dipesh ShresthaNo ratings yet
- Tokyo Guidelines 2018 Flowchart For The ManagementDocument19 pagesTokyo Guidelines 2018 Flowchart For The ManagementDipesh ShresthaNo ratings yet
- Aha Bls & Acls 2015 AlgorithmsDocument20 pagesAha Bls & Acls 2015 AlgorithmsDipesh Shrestha100% (1)
- Drug of ChoiceDocument3 pagesDrug of ChoiceDipesh ShresthaNo ratings yet
- 6 Biochemistry Map PDFDocument2 pages6 Biochemistry Map PDFDipesh ShresthaNo ratings yet
- 10 1001@jama 2016 0287Document10 pages10 1001@jama 2016 0287ompardor7554No ratings yet
- Brain Mnemonic SDocument36 pagesBrain Mnemonic SLouie OkayNo ratings yet
- ACG Guideline AcutePancreatitis September 2013Document16 pagesACG Guideline AcutePancreatitis September 2013gorditomaloNo ratings yet
- Biology Syllabus HSEBDocument2 pagesBiology Syllabus HSEBDipesh ShresthaNo ratings yet
- 200 Questions On Biology With ExplanationDocument39 pages200 Questions On Biology With ExplanationvgasNo ratings yet
- Note By4 By5Document263 pagesNote By4 By5Ae BanpongNo ratings yet
- Biology Questions and AnswersDocument472 pagesBiology Questions and Answersbusybeefreedom100% (1)
- Biology Syllabus HSEBDocument2 pagesBiology Syllabus HSEBDipesh ShresthaNo ratings yet
- 7690-3638 High School Science Biology Student Resource Book 08-09 PDFDocument240 pages7690-3638 High School Science Biology Student Resource Book 08-09 PDFGustavo KstNo ratings yet
- Shreya Keshari PDFDocument75 pagesShreya Keshari PDFANKIT SINGHNo ratings yet
- Fundamentals of Biochemical Engineering Dutta Solution ManualDocument6 pagesFundamentals of Biochemical Engineering Dutta Solution Manualhimanshu18% (22)
- GMAT2111 General Mathematics Long Quiz 2Document2 pagesGMAT2111 General Mathematics Long Quiz 2Mike Danielle AdaureNo ratings yet
- Diexis in Red by Taylor SwiftDocument11 pagesDiexis in Red by Taylor SwiftNirmana ArtstikaNo ratings yet
- PCA Power StatusDocument10 pagesPCA Power Statussanju_81No ratings yet
- Letters of ComplaintDocument3 pagesLetters of ComplaintMercedes Jimenez RomanNo ratings yet
- 145class 7 Integers CH 1Document2 pages145class 7 Integers CH 17A04Aditya MayankNo ratings yet
- Security and Azure SQL Database White PaperDocument15 pagesSecurity and Azure SQL Database White PaperSteve SmithNo ratings yet
- 1 Patient Assessment Form.Document3 pages1 Patient Assessment Form.Aina HaravataNo ratings yet
- Ingles Semana 11. P6. 2Q. 4egb. A y BDocument2 pagesIngles Semana 11. P6. 2Q. 4egb. A y BWendisilla BelenchisNo ratings yet
- WE) The Accentual Structure of English WordsDocument8 pagesWE) The Accentual Structure of English Wordszhannatagabergen2606No ratings yet
- PRS Product DescriptionDocument42 pagesPRS Product DescriptioneliaezekielNo ratings yet
- Pakistan's Professor Mafia - Pakistan - DAWNDocument5 pagesPakistan's Professor Mafia - Pakistan - DAWNMuhammad Bilal A. RNo ratings yet
- Hyrons College Philippines Inc. Sto. Niño, Tukuran, Zamboanga Del Sur SEC. No.: CN200931518 Tel. No.: 945 - 0158Document5 pagesHyrons College Philippines Inc. Sto. Niño, Tukuran, Zamboanga Del Sur SEC. No.: CN200931518 Tel. No.: 945 - 0158Mashelet Villezas ValleNo ratings yet
- ERP Test BankDocument29 pagesERP Test BankAsma 12No ratings yet
- Mactor Report - Taller de Prospectiva D 2Document39 pagesMactor Report - Taller de Prospectiva D 2Giovani Alexis Saez VegaNo ratings yet
- Assignment in Legal CounselingDocument4 pagesAssignment in Legal CounselingEmmagine E EyanaNo ratings yet
- Inheritance : Trung Tâm Anh NG Nhung PH M 27N7A KĐT Trung Hòa Nhân Chính - 0946 530 486 - 0964 177 322Document3 pagesInheritance : Trung Tâm Anh NG Nhung PH M 27N7A KĐT Trung Hòa Nhân Chính - 0946 530 486 - 0964 177 322Trung PhamNo ratings yet
- Amy Kelaidis Resume Indigeous Education 2015 FinalDocument3 pagesAmy Kelaidis Resume Indigeous Education 2015 Finalapi-292414807No ratings yet
- ContinentalDocument61 pagesContinentalSuganya RamachandranNo ratings yet
- Mission Veng 29th, 2019Document4 pagesMission Veng 29th, 2019Lasky ChhakchhuakNo ratings yet
- Assignment 1 TVM, Bonds StockDocument2 pagesAssignment 1 TVM, Bonds StockMuhammad Ali SamarNo ratings yet
- Demo StatDocument5 pagesDemo StatCalventas Tualla Khaye JhayeNo ratings yet
- S.I.M. InnovaDocument51 pagesS.I.M. InnovaPauline Karen ConcepcionNo ratings yet
- ) Mark Scheme (Results) January 2019: Pearson Edexcel International GCSE in Mathematics A (4MA1) Higher Tier Paper 1HRDocument22 pages) Mark Scheme (Results) January 2019: Pearson Edexcel International GCSE in Mathematics A (4MA1) Higher Tier Paper 1HRNewtonNo ratings yet
- Detailed Lesson Plan in Tle Grade 8Document7 pagesDetailed Lesson Plan in Tle Grade 8Hanna MikangcrzNo ratings yet
- Test Bank For Davis Advantage For Medical-Surgical Nursing: Making Connections To Practice, 2nd Edition, Janice J. Hoffman Nancy J. SullivanDocument36 pagesTest Bank For Davis Advantage For Medical-Surgical Nursing: Making Connections To Practice, 2nd Edition, Janice J. Hoffman Nancy J. Sullivannombril.skelp15v4100% (15)
- Apcr MCR 3Document13 pagesApcr MCR 3metteoroNo ratings yet
- Engineering Academy: ESE Conventional Revision TEST - IDocument8 pagesEngineering Academy: ESE Conventional Revision TEST - Ividya chakitwarNo ratings yet
- Call Option Agreement Free SampleDocument2 pagesCall Option Agreement Free Sampleapi-235666177No ratings yet