You might also like
- Practical Carotid Artery StentingFrom EverandPractical Carotid Artery StentingSumaira MacdonaldNo ratings yet
- Artigo HGF Neorologia Maio 2021Document11 pagesArtigo HGF Neorologia Maio 2021Daniela MarinhoNo ratings yet
- Aortic RegurgitationFrom EverandAortic RegurgitationJan VojacekNo ratings yet
- Cost of Extracorporeal Membrane Oxygenation: Evidence From The Rikshospitalet University Hospital, Oslo, NorwayDocument4 pagesCost of Extracorporeal Membrane Oxygenation: Evidence From The Rikshospitalet University Hospital, Oslo, NorwayArief LiemNo ratings yet
- Acute Stroke Management in the Era of ThrombectomyFrom EverandAcute Stroke Management in the Era of ThrombectomyEdgar A. SamaniegoNo ratings yet
- Echocardiography Dissertation IdeasDocument8 pagesEchocardiography Dissertation IdeasWhoCanWriteMyPaperForMeCanada100% (1)
- Coronary Artery Occlusions Diagnosed by Transthoracic DopplerDocument11 pagesCoronary Artery Occlusions Diagnosed by Transthoracic DopplerNag Mallesh RaoNo ratings yet
- Aortic Valve Bypass: Experience From Denmark: Original Article - Adult CardiacDocument5 pagesAortic Valve Bypass: Experience From Denmark: Original Article - Adult CardiacmoplkiNo ratings yet
- Endovascular Stentgraft Placement in Aortic Dissection A MetaanalysisDocument10 pagesEndovascular Stentgraft Placement in Aortic Dissection A MetaanalysisCiubuc AndrianNo ratings yet
- Characteristics and Contemporary Outcome Ventricular Septal Rupture Complicating Acute Myocardial Infarction: ClinicalDocument8 pagesCharacteristics and Contemporary Outcome Ventricular Septal Rupture Complicating Acute Myocardial Infarction: ClinicalJorge PalazzoloNo ratings yet
- Warrier 2008Document3 pagesWarrier 2008darkmatter1No ratings yet
- Grip Et Al-2018-British Journal of SurgeryDocument9 pagesGrip Et Al-2018-British Journal of SurgeryIrma SihotangNo ratings yet
- Oxygen Therapy in Suspected Acute Myocardial InfarctionDocument10 pagesOxygen Therapy in Suspected Acute Myocardial InfarctionPutri YunandaNo ratings yet
- 1 s2.0 S0929664608602041 MainDocument9 pages1 s2.0 S0929664608602041 MainEko SiswantoNo ratings yet
- Focus 1 Paper 4 Verheye Et Al 2015Document9 pagesFocus 1 Paper 4 Verheye Et Al 2015Jesson LuiNo ratings yet
- Pci Versus Cabg in Cad, Serruys (2009)Document12 pagesPci Versus Cabg in Cad, Serruys (2009)Henrique MachadoNo ratings yet
- Wetenschappelijk ArtikelDocument7 pagesWetenschappelijk Artikel5rfffgfgNo ratings yet
- Shaggy Aorta 8Document1 pageShaggy Aorta 8Eghet SilviuNo ratings yet
- Case Report Peripheral Arterial Disease Vaskular 2015Document8 pagesCase Report Peripheral Arterial Disease Vaskular 2015NovrizaL SaifulNo ratings yet
- Cardio VacDocument6 pagesCardio VacstarzecNo ratings yet
- The Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionDocument10 pagesThe Management of Severe Aortoiliac Occlusive Disease: Endovascular Therapy Rivals Open ReconstructionRobert ChristevenNo ratings yet
- J Jacc 2020 09 603Document12 pagesJ Jacc 2020 09 603Alejandro Alberto Garcia de la RochaNo ratings yet
- Contegra Study 2012Document11 pagesContegra Study 2012AkilaNo ratings yet
- Onwudike 2020Document10 pagesOnwudike 2020Han's OfficialNo ratings yet
- Sacks2018 PDFDocument13 pagesSacks2018 PDFJonathan Paucar ArévaloNo ratings yet
- Predictor Mortality EVARDocument7 pagesPredictor Mortality EVARAnneSaputraNo ratings yet
- Value of Red Blood Cell Distribution Width On Emergency Department Admission in Patients With Venous ThrombosisDocument6 pagesValue of Red Blood Cell Distribution Width On Emergency Department Admission in Patients With Venous ThrombosisJicko Street HooligansNo ratings yet
- Bedeutung Der Ultraschallkontrastmittel Im Angiologischen AlltagDocument65 pagesBedeutung Der Ultraschallkontrastmittel Im Angiologischen AlltagCharles ScottNo ratings yet
- Acute Stroke Intervention: The Heart of The Matter: SciencedirectDocument2 pagesAcute Stroke Intervention: The Heart of The Matter: SciencedirectMarianaPlataNo ratings yet
- Echocardiographic Assessment of Valve Stenosis: EAE/ASE Recommendations For Clinical PracticeDocument25 pagesEchocardiographic Assessment of Valve Stenosis: EAE/ASE Recommendations For Clinical PracticeLucy ManuriNo ratings yet
- ANGIOLOGIADocument13 pagesANGIOLOGIAAnnette ChavezNo ratings yet
- 2008 Granan The Scandinavian ACL Registries 2004-2007 Baseline EpidemiologyDocument6 pages2008 Granan The Scandinavian ACL Registries 2004-2007 Baseline EpidemiologyArmin ParavlićNo ratings yet
- Jauhari Vasc Systematic Review 2014Document19 pagesJauhari Vasc Systematic Review 2014Mary MoraNo ratings yet
- Advanced Aortic and Peripheral Endovascular Surgery FellowshipDocument8 pagesAdvanced Aortic and Peripheral Endovascular Surgery FellowshipMarisol MorenoNo ratings yet
- Jurnal InternasionalDocument15 pagesJurnal InternasionalDrizella anatasyaNo ratings yet
- Resuscitation of Endotheliopathy and Bleeding in Thoracic Aortic Dissections: The VIPER-OCTA Randomized Clinical Pilot TrialDocument8 pagesResuscitation of Endotheliopathy and Bleeding in Thoracic Aortic Dissections: The VIPER-OCTA Randomized Clinical Pilot TrialDanang Bagus UntoroNo ratings yet
- WJC 7 86Document16 pagesWJC 7 86misbahNo ratings yet
- 3 1 5 PDFDocument6 pages3 1 5 PDFpekeviNo ratings yet
- UC Irvine: Clinical Practice and Cases in Emergency MedicineDocument5 pagesUC Irvine: Clinical Practice and Cases in Emergency MedicinerifqiNo ratings yet
- Review Article: Arterial Stiffness and Renal Replacement Therapy: A Controversial TopicDocument8 pagesReview Article: Arterial Stiffness and Renal Replacement Therapy: A Controversial TopicDubravko VaničekNo ratings yet
- Automatic Measurements of Mitral Annular Plane Systolic Excursion and Velocities To Detect Left Ventricular DysfunctionDocument9 pagesAutomatic Measurements of Mitral Annular Plane Systolic Excursion and Velocities To Detect Left Ventricular DysfunctionMiguelNo ratings yet
- Journal of Clinical & Translational EndocrinologyDocument6 pagesJournal of Clinical & Translational EndocrinologyEka JuliantaraNo ratings yet
- Art 02Document8 pagesArt 02Paula Milla TorresNo ratings yet
- Treatment of CLI 2011 PDFDocument17 pagesTreatment of CLI 2011 PDFvas25No ratings yet
- Specialised Vascular Services Service Specification AdultsDocument25 pagesSpecialised Vascular Services Service Specification AdultsDr-Iyad AljuaidiNo ratings yet
- Duplex Ultrasound Scanning of Peripheral Arterial Disease of The Lower LimbDocument6 pagesDuplex Ultrasound Scanning of Peripheral Arterial Disease of The Lower Limbfristia rahmadyahNo ratings yet
- Editorial TASC IIDocument2 pagesEditorial TASC IIPitoAdhiNo ratings yet
- Valve-In-Valve-Tavi Procedure in Multivalvular DiseaseFuture Perspectives On Young PatientsDocument7 pagesValve-In-Valve-Tavi Procedure in Multivalvular DiseaseFuture Perspectives On Young PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Nejmoa2107727-Alteplase in StrokeDocument12 pagesNejmoa2107727-Alteplase in Stroketommy taylor084No ratings yet
- Crucial Roles of Vascular Surgeons in OncovascularDocument8 pagesCrucial Roles of Vascular Surgeons in OncovascularMatias Jurado ChaconNo ratings yet
- Yang 2018Document7 pagesYang 2018Robert ChristevenNo ratings yet
- Nejm Achiles Surgery Vs NonDocument12 pagesNejm Achiles Surgery Vs NonShandy MahardikaNo ratings yet
- (19330693 - Journal of Neurosurgery) Neuroendoscopic Stent Placement For Cerebrospinal Fluid Pathway Obstructions in AdultsDocument9 pages(19330693 - Journal of Neurosurgery) Neuroendoscopic Stent Placement For Cerebrospinal Fluid Pathway Obstructions in AdultsVlad VPNo ratings yet
- 590 80MI Definition - EHJ2007EN PDFDocument14 pages590 80MI Definition - EHJ2007EN PDFEdgar Mollinedo EscaleraNo ratings yet
- Arthroplasty As Primary Treatment For Distal Humeral Fractures Produces Reliable Results With Regards To Revisions and Adverse Events A Registry-Based Study2019Document7 pagesArthroplasty As Primary Treatment For Distal Humeral Fractures Produces Reliable Results With Regards To Revisions and Adverse Events A Registry-Based Study2019camilaNo ratings yet
- Comparison of Patients With and Without Digital Ulcers in Systemic Sclerosis: Detection of Possible Risk FactorsDocument10 pagesComparison of Patients With and Without Digital Ulcers in Systemic Sclerosis: Detection of Possible Risk Factorslol2easyNo ratings yet
- PCI StrategyDocument14 pagesPCI StrategyJason WinathaNo ratings yet
- Nonoperative or Surgical Treatment of Acute Achille's Tendon Rupture NEJM 2022Document12 pagesNonoperative or Surgical Treatment of Acute Achille's Tendon Rupture NEJM 2022Americo BarbosaNo ratings yet
- Granata 2015Document2 pagesGranata 2015Arthur AlbertNo ratings yet
- Clinical Review: Hemodynamic Monitoring in The Intensive Care UnitDocument8 pagesClinical Review: Hemodynamic Monitoring in The Intensive Care Unitmasfak97No ratings yet
- HEMATOLOGY-LECTURE-NOTES FTP Lectures PDFDocument50 pagesHEMATOLOGY-LECTURE-NOTES FTP Lectures PDFkat100% (8)
- Mplsheartjournal D 17 00004Document6 pagesMplsheartjournal D 17 00004Irina NeamtuNo ratings yet
- Managementul Pacientilor Boala Arteriala PerifericaDocument5 pagesManagementul Pacientilor Boala Arteriala PerifericaIrina NeamtuNo ratings yet
- Mplsheartjournal D 17 00004Document6 pagesMplsheartjournal D 17 00004Irina NeamtuNo ratings yet
- 1218 Anexa 15 - 8724 - 6616Document9 pages1218 Anexa 15 - 8724 - 6616Irina NeamtuNo ratings yet
- Pi Is 0741521414007095Document12 pagesPi Is 0741521414007095Irina NeamtuNo ratings yet
- Epidemiology of Peripheral Artery DiseaseDocument18 pagesEpidemiology of Peripheral Artery DiseaseIrina NeamtuNo ratings yet
- Incidence of Peripheral Vascular Changes in Diabetes MellitusDocument5 pagesIncidence of Peripheral Vascular Changes in Diabetes MellitusIrina NeamtuNo ratings yet
- ESC Guidelines Peripheral Arterial Diseases 2017Document9 pagesESC Guidelines Peripheral Arterial Diseases 2017Irina NeamtuNo ratings yet
- ESC Guidelines Peripheral Arterial Diseases 2017Document9 pagesESC Guidelines Peripheral Arterial Diseases 2017Irina NeamtuNo ratings yet
- Complications After Peripheral Vascular Interventions in OctogenariansDocument7 pagesComplications After Peripheral Vascular Interventions in OctogenariansIrina NeamtuNo ratings yet
- Population-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial EventsDocument11 pagesPopulation-Based Study of Incidence, Risk Factors, Outcome, and Prognosis of Ischemic Peripheral Arterial EventsIrina NeamtuNo ratings yet
- Pneumonia NosocomialaDocument6 pagesPneumonia NosocomialaAriana CordoșNo ratings yet
- CTG HaDocument15 pagesCTG HaNabila SaribanunNo ratings yet
- Endocrine VARIANTA 2Document2 pagesEndocrine VARIANTA 2Irina NeamtuNo ratings yet
- Pneumologie Subiecte ExamenDocument6 pagesPneumologie Subiecte ExamenSanda BuruianăNo ratings yet
- Cap 1 Introduce Re)Document2 pagesCap 1 Introduce Re)vlad910No ratings yet
- Anatomy Orbit and Eyelid - WashedDocument1 pageAnatomy Orbit and Eyelid - WashedIrina NeamtuNo ratings yet
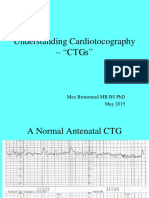
- Understanding Cardiotocography - "CTGS": Max Brinsmead MB Bs PHD May 2015Document29 pagesUnderstanding Cardiotocography - "CTGS": Max Brinsmead MB Bs PHD May 2015Irina NeamtuNo ratings yet
- 24Document485 pages24Irina Neamtu100% (1)
- Profilax TBCDocument2 pagesProfilax TBCIrina NeamtuNo ratings yet
- BOMSS Standards For Clinical ServicesDocument4 pagesBOMSS Standards For Clinical ServiceskintNo ratings yet
- CsaDocument10 pagesCsaBEATRIZ CUBILLONo ratings yet
- Basic Nursing:Foundations of Skills & Concepts: Diagnostic TestsDocument41 pagesBasic Nursing:Foundations of Skills & Concepts: Diagnostic TestsellaguraNo ratings yet
- Asymptomatic TransaminitisDocument2 pagesAsymptomatic TransaminitisrieseNo ratings yet
- Persuasive LetterDocument2 pagesPersuasive Letterapi-341527188No ratings yet
- Working For A: #Hepfreefuture by 2030Document2 pagesWorking For A: #Hepfreefuture by 2030Mya MyintzuNo ratings yet
- Perforative PeritonitisDocument58 pagesPerforative PeritonitisSangeeta BSR82% (17)
- Gene Therapy: by Prof. Liwayway Memije-CruzDocument12 pagesGene Therapy: by Prof. Liwayway Memije-CruzMarie WongNo ratings yet
- Risk Benefit Evaluation For Bicalutamide Bouvy2016Document11 pagesRisk Benefit Evaluation For Bicalutamide Bouvy2016Mary FallNo ratings yet
- BMJ 334 7593 CR 00579Document10 pagesBMJ 334 7593 CR 00579RonaMaulidiaBakhitaNo ratings yet
- FDA Inspection in India (2005 - 2012)Document11 pagesFDA Inspection in India (2005 - 2012)Asijit SenNo ratings yet
- Crohn's DiseaseDocument14 pagesCrohn's Diseasevenzmartinez100% (1)
- Guidelines Village WSCDocument20 pagesGuidelines Village WSCvenkatasubramaniyanNo ratings yet
- 70 150 1 SM PDFDocument9 pages70 150 1 SM PDFUsbahNo ratings yet
- The Active Pharmaceutical Ingredients (API) MarketDocument5 pagesThe Active Pharmaceutical Ingredients (API) Marketlek01No ratings yet
- Musculoskeletal Disorders Part 1 Metabolic Bone Disorders.Document84 pagesMusculoskeletal Disorders Part 1 Metabolic Bone Disorders.Carmela Lacsa DomocmatNo ratings yet
- Kaur, Diabetic Autonomic Neuropathy Pathogenesis and Treatment, 2014Document8 pagesKaur, Diabetic Autonomic Neuropathy Pathogenesis and Treatment, 2014elbueno21No ratings yet
- Lesson 7. Education, Religion, Belief System and Health - StudentDocument49 pagesLesson 7. Education, Religion, Belief System and Health - StudentAhyessa Castillo100% (1)
- GRH D 16 00001 ManuscriptDocument224 pagesGRH D 16 00001 ManuscriptsrividyargNo ratings yet
- Obstetric Guidelines 2017Document288 pagesObstetric Guidelines 2017susnari100% (1)
- The Rolle of Surgery in Oncology: Surgery Departement Medical Faculty Ukrida UniversityDocument25 pagesThe Rolle of Surgery in Oncology: Surgery Departement Medical Faculty Ukrida UniversityGian Alodia RisamasuNo ratings yet
- ENDOCRINE 1.3 Incidentallomas, Conn's SyndromeDocument5 pagesENDOCRINE 1.3 Incidentallomas, Conn's SyndromeJem QuintoNo ratings yet
- The Sight Vol. 5Document60 pagesThe Sight Vol. 5optometrynepalNo ratings yet
- Veterinary DiagnosisDocument2 pagesVeterinary Diagnosissuscripciones.meNo ratings yet
- Revison de Proyecto Tunning LatinoamericaDocument13 pagesRevison de Proyecto Tunning LatinoamericaJorge Solar RosselNo ratings yet
- Links To Clinical Info About The VaccineDocument9 pagesLinks To Clinical Info About The VaccinekarunaNo ratings yet
- Music I. Read The Following Questions Carefully and Write The Letter of The Correct Answer On Your Answer SheetDocument4 pagesMusic I. Read The Following Questions Carefully and Write The Letter of The Correct Answer On Your Answer SheetJohn Christopher Ping-ay Par IINo ratings yet
- Down SyndromeDocument20 pagesDown SyndromeJessa DiñoNo ratings yet
- IS - Safe T Centesis Catheter Drainage - BR - ENDocument6 pagesIS - Safe T Centesis Catheter Drainage - BR - ENMalekseuofi مالك السيوفيNo ratings yet
- Doctors Email DataDocument11 pagesDoctors Email DataNaveenJainNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingFrom EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingRating: 4 out of 5 stars4/5 (1138)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsFrom EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsRating: 4.5 out of 5 stars4.5/5 (6)