You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Mpac Sept2016 World Malaria ReportDocument19 pagesMpac Sept2016 World Malaria ReporttriNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Current Management and Treatment of Dry Eye Disease: ReviewDocument5 pagesCurrent Management and Treatment of Dry Eye Disease: ReviewtriNo ratings yet
- 452 883 1 SM PDFDocument7 pages452 883 1 SM PDFsri marianaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 1-Wayan Getas-Juni 2012 PDFDocument6 pages1-Wayan Getas-Juni 2012 PDFtriNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- MWJ2016 7 3Document6 pagesMWJ2016 7 3triNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Global Vector Control Response 2017-2030: Fourth Draft (Version 4.3)Document50 pagesGlobal Vector Control Response 2017-2030: Fourth Draft (Version 4.3)Febby WadoeNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Saillant 2019Document9 pagesSaillant 2019triNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Micheletti2018 PDFDocument67 pagesMicheletti2018 PDFtriNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- C2eek635 BYCDocument65 pagesC2eek635 BYCtriNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Risk Perception Regarding Drug Use in PregnancyDocument4 pagesRisk Perception Regarding Drug Use in PregnancytriNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Micheletti2018 PDFDocument67 pagesMicheletti2018 PDFtriNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 1 s2.0 S0002937819307069 Main PDFDocument13 pages1 s2.0 S0002937819307069 Main PDFtriNo ratings yet
- Host-Seeking Activity of A Tanzanian Population of Anopheles Arabiensis at An Insecticide Treated Bed NetDocument14 pagesHost-Seeking Activity of A Tanzanian Population of Anopheles Arabiensis at An Insecticide Treated Bed NettriNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Saillant 2019Document9 pagesSaillant 2019triNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Stroumsa 2019Document4 pagesStroumsa 2019triNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 97165673-f831-4abe-a55b-dd9862e49200Document5 pages97165673-f831-4abe-a55b-dd9862e49200triNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Bogani Et Al-2019-International Journal of Gynecology & Obstetrics PDFDocument5 pagesBogani Et Al-2019-International Journal of Gynecology & Obstetrics PDFtriNo ratings yet
- 97165673-f831-4abe-a55b-dd9862e49200Document5 pages97165673-f831-4abe-a55b-dd9862e49200triNo ratings yet
- Anatomical and Pathophysiological Classification of Congenital Heart DiseaseDocument16 pagesAnatomical and Pathophysiological Classification of Congenital Heart DiseasePietro PensoNo ratings yet
- Saillant 2019Document9 pagesSaillant 2019triNo ratings yet
- 1 s2.0 S0002937819307069 Main PDFDocument13 pages1 s2.0 S0002937819307069 Main PDFtriNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Bogani Et Al-2019-International Journal of Gynecology & ObstetricsDocument5 pagesBogani Et Al-2019-International Journal of Gynecology & ObstetricstriNo ratings yet
- 1 s2.0 S0002937819306817 MainDocument11 pages1 s2.0 S0002937819306817 MaintriNo ratings yet
- E81 FullDocument112 pagesE81 FulltriNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Stroumsa 2019Document4 pagesStroumsa 2019triNo ratings yet
- 1 s2.0 S107476131500179X MainDocument13 pages1 s2.0 S107476131500179X MaintriNo ratings yet
- 1 s2.0 S0002937819307069 Main PDFDocument13 pages1 s2.0 S0002937819307069 Main PDFtriNo ratings yet
- Menopausal Symptoms and Surgical Complications After Opportunistic Bilateral Salpingectomy, A Register-Based Cohort StudyDocument10 pagesMenopausal Symptoms and Surgical Complications After Opportunistic Bilateral Salpingectomy, A Register-Based Cohort StudytriNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- 1 s2.0 S107476131500179X MainDocument13 pages1 s2.0 S107476131500179X MaintriNo ratings yet
- 1 s2.0 S0002937819306817 MainDocument11 pages1 s2.0 S0002937819306817 MaintriNo ratings yet
- Indications of General Anaesthesia in Dentistry 3Document2 pagesIndications of General Anaesthesia in Dentistry 3NaseemNo ratings yet
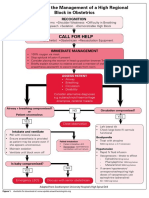
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- NailSurgery With Name ChangesDocument55 pagesNailSurgery With Name ChangesIde Bagoes InsaniNo ratings yet
- Jurnal Reading Rizki Widya Kirana - 03012236Document15 pagesJurnal Reading Rizki Widya Kirana - 03012236R Widya KiranaNo ratings yet
- Endodontics Pain Control in Endodontics: Differential Diagnosis of Dental PainDocument4 pagesEndodontics Pain Control in Endodontics: Differential Diagnosis of Dental Painريام الموسويNo ratings yet
- Medical EmergenciesDocument115 pagesMedical EmergenciesRamya ReddyNo ratings yet
- Geriatrics Quiz 10 QuestionsDocument2 pagesGeriatrics Quiz 10 QuestionsBrian Strauss100% (4)
- La Management of Special PtientDocument27 pagesLa Management of Special PtientIyad Abou-RabiiNo ratings yet
- Pharmacology: General Anaesthetic AgentsDocument65 pagesPharmacology: General Anaesthetic AgentsSharifa DarayanNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Dental Anestesi Jurnal 2Document2 pagesDental Anestesi Jurnal 2Indira NoormaliyaNo ratings yet
- Rocuronium: Bromide InjectionDocument2 pagesRocuronium: Bromide InjectionNursalfarinah BasirNo ratings yet
- PharmacologyDocument236 pagesPharmacologynbde2100% (5)
- Recommendations To Use Vasoconstrictors in Dentistry and Oral SurgeryDocument30 pagesRecommendations To Use Vasoconstrictors in Dentistry and Oral SurgeryAnonymous i7fNNiRqh2No ratings yet
- Local Anesthetic Systemic Toxicity AlgorithmDocument1 pageLocal Anesthetic Systemic Toxicity AlgorithmSydney JenningsNo ratings yet
- Bedah Buku InstrumenDocument12 pagesBedah Buku Instrumencoffe latteNo ratings yet
- DR - Vinay Jain PG1 YearDocument76 pagesDR - Vinay Jain PG1 YearNeelesh BhatnagarNo ratings yet
- Sural Nerve BiopsyDocument2 pagesSural Nerve BiopsyArindam MukherjeeNo ratings yet
- MCQs LADocument29 pagesMCQs LAPadmavathi C100% (1)
- Pharma MCQDocument0 pagesPharma MCQFoysal Sirazee0% (2)
- Spinal and Epidural Anesthesia: Jedarlyn G. Erardo, RPH, MDDocument101 pagesSpinal and Epidural Anesthesia: Jedarlyn G. Erardo, RPH, MDjedarlynNo ratings yet
- Caesarean in Mare by Marcenac Incision Under Local AnaesthesiaDocument3 pagesCaesarean in Mare by Marcenac Incision Under Local AnaesthesiaDanielaNo ratings yet
- Buffered Anaesthetic S: DR Shazeena QaiserDocument25 pagesBuffered Anaesthetic S: DR Shazeena QaiserShazeena OfficialNo ratings yet
- Perioperative Nursing - OrIGINALDocument176 pagesPerioperative Nursing - OrIGINALJamil Lorca100% (4)
- Hialuronidasa en Bloqueo AxilarDocument8 pagesHialuronidasa en Bloqueo Axilarantonio123valenciaNo ratings yet
- Anesthetics - They Decrease Afferent Nerves Sensibility B.astringent, C.covering, D.adsorbingDocument4 pagesAnesthetics - They Decrease Afferent Nerves Sensibility B.astringent, C.covering, D.adsorbingAnjaliNo ratings yet
- Meralgia ParestheticaDocument22 pagesMeralgia ParestheticaWahyu Tri KusprasetyoNo ratings yet
- Local Anesthetics: Ms. Sneha J. SawantDocument11 pagesLocal Anesthetics: Ms. Sneha J. Sawantrushikesh ugaleNo ratings yet
- Local AnestheticsDocument47 pagesLocal AnestheticsKeerthi LakshmiNo ratings yet
- Use This File If Printing The Whole WorkbookDocument819 pagesUse This File If Printing The Whole WorkbookAndrewNo ratings yet
- Saddle BlockDocument3 pagesSaddle BlockVasu DevanNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)