You might also like
- Dermatology Essentials for Medical AssistantsFrom EverandDermatology Essentials for Medical AssistantsRating: 4 out of 5 stars4/5 (1)
- Dermatology EssentialsDocument1,037 pagesDermatology EssentialsViviana Malaver Yepes100% (8)
- General Dermatology MCQsDocument197 pagesGeneral Dermatology MCQsDr.Tawheed95% (19)
- MCQ DermatologyDocument2 pagesMCQ DermatologyDr.Tawheed100% (7)
- Dermatology MCQ FRCPDocument101 pagesDermatology MCQ FRCPhesham89% (19)
- Vesicular and Bullous Dermatosis MCQsDocument59 pagesVesicular and Bullous Dermatosis MCQsDr.Tawheed88% (8)
- Anatomy Multiple Choice & Short Answer QuestionsDocument3 pagesAnatomy Multiple Choice & Short Answer QuestionsFaddy Oraha74% (23)
- Muscles of The Upper Limb Made EasyDocument7 pagesMuscles of The Upper Limb Made Easynss92% (26)
- Med Dermatology Questions-75Document67 pagesMed Dermatology Questions-75Khalifa AL-Wishahi75% (4)
- Derma MCQ Ch01Document20 pagesDerma MCQ Ch01Rasha Dabbagh75% (4)
- Photodermatology MCQsDocument53 pagesPhotodermatology MCQsDr.Tawheed100% (8)
- MCQs in Pharmacology PDFDocument244 pagesMCQs in Pharmacology PDFandirio748690% (10)
- Dermatology QuizDocument10 pagesDermatology QuizSyed Ali Haider0% (1)
- DermatologyDocument3 pagesDermatologyDrkhslid890% (1)
- Genodermatosis MCQsDocument152 pagesGenodermatosis MCQsDr.Tawheed88% (8)
- ETAS MCQ 2015 - Derm-In-Review Volume 1Document672 pagesETAS MCQ 2015 - Derm-In-Review Volume 1Muhammad Javed Gaba100% (1)
- Reading 2019 FoundationDocument16 pagesReading 2019 FoundationFaddy OrahaNo ratings yet
- C3 Differentiation Topic AssessmentDocument6 pagesC3 Differentiation Topic AssessmentFaddy OrahaNo ratings yet
- GI Anatomy Practice QuestionsDocument6 pagesGI Anatomy Practice QuestionsFaddy OrahaNo ratings yet
- Case Analysis Tool Worksheet: Squamous Cell CarcinomaDocument4 pagesCase Analysis Tool Worksheet: Squamous Cell CarcinomaDina KristevaNo ratings yet
- Eczema (Dermatitis), Atopic Dermatitis, Seborrhoeic DermatitisDocument25 pagesEczema (Dermatitis), Atopic Dermatitis, Seborrhoeic DermatitisAtqiya Maisha LataNo ratings yet
- Red and green skin answers keyDocument9 pagesRed and green skin answers keyNiwashiny CnyNo ratings yet
- Dermatology QuestionsDocument3 pagesDermatology QuestionsMuziki Wa KiafrikaNo ratings yet
- Dermatopathology Q - ADocument55 pagesDermatopathology Q - AKhalifa AL-Wishahi100% (7)
- Pediatric Dermatology MCQsDocument53 pagesPediatric Dermatology MCQsDr.Tawheed89% (18)
- Part I 2016 - Dermatology MCQDocument9 pagesPart I 2016 - Dermatology MCQEmma Dawod100% (1)
- 11Document3 pages11faresaltaii100% (2)
- Dermatology MCQ With AnswersDocument27 pagesDermatology MCQ With Answershesham0% (1)
- Mcqs of Icthyosis With KeyDocument7 pagesMcqs of Icthyosis With KeysaleemNo ratings yet
- MCQ DermatologyDocument42 pagesMCQ Dermatologydraik71100% (5)
- MCQs Ch07-45651100rdzDocument27 pagesMCQs Ch07-45651100rdzKhalifa AL-Wishahi100% (2)
- Dermatology Written Exam 2007Document6 pagesDermatology Written Exam 2007Abdullah Matar BadranNo ratings yet
- Derma CD McqsDocument22 pagesDerma CD McqsheshamNo ratings yet
- MCQ IN DERMATOLOGY NMT 08 - مركز إبن الاسلام ... (20ebooks.com)Document17 pagesMCQ IN DERMATOLOGY NMT 08 - مركز إبن الاسلام ... (20ebooks.com)R Ratheesh100% (9)
- DermatologyDocument17 pagesDermatologyEbn Seena75% (4)
- MCQ Dermatology (Dr. Asaf K.)Document31 pagesMCQ Dermatology (Dr. Asaf K.)Dinesh JadhavNo ratings yet
- Key Skin ConditionsDocument8 pagesKey Skin Conditionsfairodz salapudinNo ratings yet
- End Round of Dermatology, MCQsDocument20 pagesEnd Round of Dermatology, MCQsMuhdZaeed100% (2)
- 101-Normal Skin MCQsDocument25 pages101-Normal Skin MCQsHybat ElsheikhNo ratings yet
- Prometric Book 2nd EditionDocument207 pagesPrometric Book 2nd Editionsajitha100% (1)
- Dermatology Finals (Sept. 2014)Document14 pagesDermatology Finals (Sept. 2014)Paz VidaNo ratings yet
- 1-Dermatological Case PresentationDocument41 pages1-Dermatological Case Presentationnaimat007No ratings yet
- Dermatoven MCQDocument30 pagesDermatoven MCQS2 GIZI FKUI 2020No ratings yet
- DermatologyDocument121 pagesDermatologyjimisurgon83100% (4)
- Dermatology MCQ With ExplinationsDocument46 pagesDermatology MCQ With ExplinationsheshamNo ratings yet
- Dermatology Postgraduate MCQs and Revision Notes2Document56 pagesDermatology Postgraduate MCQs and Revision Notes2hesham50% (2)
- Photo QuizDocument21 pagesPhoto Quizabas_maytham1021100% (3)
- Dermatology Skin Conditions and TreatmentsDocument8 pagesDermatology Skin Conditions and TreatmentsMichael NyaataNo ratings yet
- Skin MCQ Wo AnsDocument2 pagesSkin MCQ Wo Anssmbawasaini100% (1)
- PSORIASIS STUDY GUIDEDocument5 pagesPSORIASIS STUDY GUIDEhesham100% (4)
- Derma MCQ Ch01 PDFDocument20 pagesDerma MCQ Ch01 PDFShah NawazNo ratings yet
- Final Exam One Answered 2.. All 3 VersionsDocument21 pagesFinal Exam One Answered 2.. All 3 Versionsh8j5fnyh7dNo ratings yet
- June 2022 - Dermatology - 10 McqsDocument8 pagesJune 2022 - Dermatology - 10 McqsAhmed ShihataNo ratings yet
- Cutaneous Manifestations of Tuberous SclerosisDocument5 pagesCutaneous Manifestations of Tuberous SclerosisRavva0% (1)
- KONCPT NEET PG GRAND TESTDocument48 pagesKONCPT NEET PG GRAND TESTSonalNo ratings yet
- Derma FinalDocument5 pagesDerma FinalMr.FantasthiccNo ratings yet
- Dermatology EMQDocument4 pagesDermatology EMQislamawniNo ratings yet
- 125 TOP DERMATOLOGY MULTIPLE CHOICE QUESTIONS AND ANSWERSDocument30 pages125 TOP DERMATOLOGY MULTIPLE CHOICE QUESTIONS AND ANSWERSMuha RajNo ratings yet
- Genodermatoses and Vascular MalformationsDocument60 pagesGenodermatoses and Vascular Malformationsalh bashar100% (1)
- Prometric Exam March 2020Document250 pagesPrometric Exam March 2020Sally dossNo ratings yet
- Pics MCQSDocument22 pagesPics MCQStaniaNo ratings yet
- Immunedermatology MCQsDocument73 pagesImmunedermatology MCQsDr.Tawheed90% (10)
- Dermatology RecertificatDocument8 pagesDermatology RecertificatKhalifa AL-WishahiNo ratings yet
- Dermat Questions 252Document72 pagesDermat Questions 252Srirupa BiswasNo ratings yet
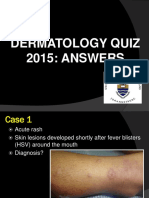
- Dermatology Quiz 2015 AnswersDocument40 pagesDermatology Quiz 2015 Answerspoorva shahNo ratings yet
- Rubin Skin Review Q's&a'sDocument7 pagesRubin Skin Review Q's&a'sJUSASBNo ratings yet
- Leg, Arm, and Chest Papules: ERM ASEDocument9 pagesLeg, Arm, and Chest Papules: ERM ASEdeenutz93No ratings yet
- Demonstrative NounsDocument17 pagesDemonstrative NounsFaddy OrahaNo ratings yet
- Orbital TumorsDocument68 pagesOrbital TumorsFaddy OrahaNo ratings yet
- Rossana ABC L 1 Reading and Writting Exam PapaerDocument2 pagesRossana ABC L 1 Reading and Writting Exam PapaerFaddy OrahaNo ratings yet
- Adrenergic Neurotransmitter PDFDocument4 pagesAdrenergic Neurotransmitter PDFFaddy OrahaNo ratings yet
- Demonstrative Pronouns in English and ArabicDocument13 pagesDemonstrative Pronouns in English and ArabicFaddy OrahaNo ratings yet
- Article AVI in UKDocument10 pagesArticle AVI in UKFaddy OrahaNo ratings yet
- Adjectives in English and ArabicDocument7 pagesAdjectives in English and ArabicFaddy OrahaNo ratings yet
- IAL Mathematics Sample Assessment MaterialDocument460 pagesIAL Mathematics Sample Assessment MaterialMohamed Naaif100% (3)
- Italian Sommario Translated Gastro&EndoDocument33 pagesItalian Sommario Translated Gastro&EndoFaddy OrahaNo ratings yet
- Presentation 1Document4 pagesPresentation 1Faddy OrahaNo ratings yet
- Aspirin Is - AnalgesicDocument2 pagesAspirin Is - AnalgesicFaridOrahaNo ratings yet
- The EpidemiologyDocument15 pagesThe EpidemiologyFaddy OrahaNo ratings yet
- Carbon Fixation Teacher NotesDocument2 pagesCarbon Fixation Teacher NotesLesley BoultonNo ratings yet
- Amount of Substance Aspirin Calculation Year 12Document6 pagesAmount of Substance Aspirin Calculation Year 12FaridOrahaNo ratings yet
- Exam III 2014Document10 pagesExam III 2014Faddy OrahaNo ratings yet
- Edexcel - Core 3 and 4 Revision SheetDocument6 pagesEdexcel - Core 3 and 4 Revision SheetAshraf Uz ZamanNo ratings yet
- Introduzione Alla Farmacologia - It.enDocument3 pagesIntroduzione Alla Farmacologia - It.enFaddy OrahaNo ratings yet
- Edexcel C3 QP Jan 2011Document28 pagesEdexcel C3 QP Jan 2011Issam SaifNo ratings yet
- c3.3 Trigonometry 1Document35 pagesc3.3 Trigonometry 1Faddy OrahaNo ratings yet
- Drug DiscoveryDocument29 pagesDrug DiscoveryFaddy OrahaNo ratings yet
- T Dev 230417-EDocument78 pagesT Dev 230417-EFaddy OrahaNo ratings yet
- Sample Exam 1 Embryology MCQDocument3 pagesSample Exam 1 Embryology MCQFaddy Oraha82% (11)
- Protein SortingDocument33 pagesProtein SortingFaddy Oraha100% (1)
- Search Skinaqua Watsons SingaporeDocument1 pageSearch Skinaqua Watsons SingaporeyrotnapNo ratings yet
- Oral UlcersDocument141 pagesOral UlcersKamal-Eldin Ahmed Abou-Elhamd100% (1)
- 800 Ebook Dermatology and DiabetesDocument115 pages800 Ebook Dermatology and DiabetesAhmad ArifNo ratings yet
- Part I Travel Documents Issued by Third Countries and Territorial Entities en 0Document124 pagesPart I Travel Documents Issued by Third Countries and Territorial Entities en 0drlazyboyNo ratings yet
- First Edition ReviewDocument2 pagesFirst Edition ReviewFlorin VladNo ratings yet
- Efektifitas Antibiotik Azelaic Acid TerhDocument12 pagesEfektifitas Antibiotik Azelaic Acid TerhSILVY CINTIYA DEWINo ratings yet
- PERSONAL CARE EnglishDocument7 pagesPERSONAL CARE EnglishDio SamputraNo ratings yet
- Blistering DiseasesDocument26 pagesBlistering DiseasesLia-Maria BufteaNo ratings yet
- Psoriasis Dermatitis FinalDocument50 pagesPsoriasis Dermatitis Finalapi-546809761No ratings yet
- Full Urticaria Cure by DR GaryDocument2 pagesFull Urticaria Cure by DR GaryMishu DianaNo ratings yet
- Mcqs of Icthyosis With KeyDocument7 pagesMcqs of Icthyosis With KeysaleemNo ratings yet
- Avoskin, Vavl Beaute, True to Skin and More Skincare PricelistsDocument6 pagesAvoskin, Vavl Beaute, True to Skin and More Skincare PricelistsVivian LieNo ratings yet
- Scarless Silicone Gel BrochureDocument6 pagesScarless Silicone Gel BrochureKhaled SalahNo ratings yet
- Dermoscopy of Disorders of HypopigmentationDocument5 pagesDermoscopy of Disorders of HypopigmentationIJAR JOURNALNo ratings yet
- Screenshot 2023-01-09 at 11.14.21Document18 pagesScreenshot 2023-01-09 at 11.14.21yahya aburmailehNo ratings yet
- Brosur Nectars 2022 PDFDocument3 pagesBrosur Nectars 2022 PDFLeon Firdaus IkhsanNo ratings yet
- 1234Document222 pages1234NDTV100% (1)
- Derm Quick ReviewDocument124 pagesDerm Quick ReviewRohit NalamasuNo ratings yet
- Shades by Kolours: Week #: Period CoveredDocument5 pagesShades by Kolours: Week #: Period CoveredChristian TerribleNo ratings yet
- Stok OpnameDocument262 pagesStok OpnamenailifinaNo ratings yet
- Moluscum ContagiosumDocument6 pagesMoluscum ContagiosumngurahdwikyNo ratings yet
- Classification of White Oral LesionsDocument32 pagesClassification of White Oral LesionsMira Anggriani100% (1)
- Pharmacy Order ListingDocument13 pagesPharmacy Order ListingAlex NaranjoNo ratings yet
- Last Aid Dermatology SARPDocument7 pagesLast Aid Dermatology SARPskNo ratings yet
- How To Describe Skin Rash PDFDocument72 pagesHow To Describe Skin Rash PDFGabrijela PejkićNo ratings yet
- Analisa Asam SalisilatDocument5 pagesAnalisa Asam SalisilatMahardikaNo ratings yet
- Your Daytime Regimen: Step 1: CleanserDocument2 pagesYour Daytime Regimen: Step 1: CleanserJay GrijaldoNo ratings yet