You might also like
- Hip Survey A3 Poster WEBDocument1 pageHip Survey A3 Poster WEBvictor_venki9955No ratings yet
- Hip Surveillance PathwayDocument2 pagesHip Surveillance PathwaymiguelpaillalefgutierrezNo ratings yet
- Simplified Blood Pressuretable: Full BP Tables ArecomplicatedDocument14 pagesSimplified Blood Pressuretable: Full BP Tables ArecomplicatedaaNo ratings yet
- Policy: Nevada WIC Program-Certification Page 1 of 6Document6 pagesPolicy: Nevada WIC Program-Certification Page 1 of 6TanveerNo ratings yet
- Heartworm Disease: What To Do With Your SNAP ResultDocument1 pageHeartworm Disease: What To Do With Your SNAP ResultIantela AlexNo ratings yet
- NIV Algorithm Final Version Jan 2020Document3 pagesNIV Algorithm Final Version Jan 2020AmalNo ratings yet
- Cervical Screening Care Pathway: Gov - UkDocument13 pagesCervical Screening Care Pathway: Gov - Ukbm5q2h9xbhNo ratings yet
- Appendix 2 Colposcopy ManagementDocument2 pagesAppendix 2 Colposcopy ManagementFA KhanNo ratings yet
- Meningitis Protocole المعدل 1-2-2016Document3 pagesMeningitis Protocole المعدل 1-2-2016Hamza El-ȜfifiNo ratings yet
- Recommendations For Oral Surgery During COVID-19 Pandemic: WWW - Rcseng.ac - Uk/dental-Faculties/fds/coronavirusDocument7 pagesRecommendations For Oral Surgery During COVID-19 Pandemic: WWW - Rcseng.ac - Uk/dental-Faculties/fds/coronavirusFaiqotul KumalaNo ratings yet
- Diagnosis and Management of Complete Kawasaki Disease in ChildrenDocument13 pagesDiagnosis and Management of Complete Kawasaki Disease in ChildrenJ SNo ratings yet
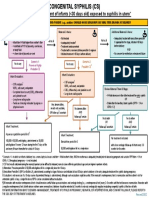
- Congenital Syphilis - Algorithm-110919-1Document1 pageCongenital Syphilis - Algorithm-110919-1Kamrul AhsanNo ratings yet
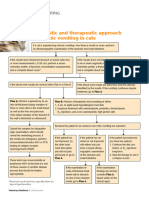
- Chronic Vomiting in CatsDocument1 pageChronic Vomiting in CatsDalia ExtrapolisNo ratings yet
- NCPDocument6 pagesNCPunkown userNo ratings yet
- Study AuditDocument28 pagesStudy Audithj ndukaNo ratings yet
- Apache ScoreDocument3 pagesApache ScoresintachscNo ratings yet
- Appeal GuidelinesDocument4 pagesAppeal GuidelinesKOONo ratings yet
- Prado, Catherine BSN IIB (Activity 1 Case Scenario)Document52 pagesPrado, Catherine BSN IIB (Activity 1 Case Scenario)Catherine PradoNo ratings yet
- KISS NewNationalCervicalScreeningProgram Feb2019Document3 pagesKISS NewNationalCervicalScreeningProgram Feb2019sahz87No ratings yet
- Covid Neo2Document1 pageCovid Neo2CHIERBEENo ratings yet
- HIV PEP-PrEPDocument2 pagesHIV PEP-PrEPSubhasish BarikNo ratings yet
- DocumentDocument1 pageDocumentHimanshuNo ratings yet
- AASLD Recommendations For HCVDocument45 pagesAASLD Recommendations For HCVRamy ElbarodyNo ratings yet
- Secondary SyphilisDocument2 pagesSecondary SyphilisRoberto López MataNo ratings yet
- Comparison of Efficacy of Gabapentin and Pregabalin in Reducing Pain Intensity in Children With Guillain Barre Syndrome 4-18 Years of Age: A Single Blind Randomized Controlled TrialDocument20 pagesComparison of Efficacy of Gabapentin and Pregabalin in Reducing Pain Intensity in Children With Guillain Barre Syndrome 4-18 Years of Age: A Single Blind Randomized Controlled TrialPrateek Kumar PandaNo ratings yet
- Algorithmforrevisedguidelinesforinternationalarrivals 30 TH November 2021Document1 pageAlgorithmforrevisedguidelinesforinternationalarrivals 30 TH November 2021Ashton KryzanowskiNo ratings yet
- Algorithmforrevisedguidelinesforinternationalarrivals 30 TH November 2021Document1 pageAlgorithmforrevisedguidelinesforinternationalarrivals 30 TH November 2021Het NandaaanaNo ratings yet
- AJCP / Special Article: BackgroundDocument27 pagesAJCP / Special Article: BackgroundnuvitaNo ratings yet
- Breastfeeding Experience in Inborn Errors of Metabolism Other Than PhenylketonuriaDocument9 pagesBreastfeeding Experience in Inborn Errors of Metabolism Other Than PhenylketonuriaRio Michelle CorralesNo ratings yet
- October 2017 Ed Infant Fever 29-60 DaysDocument4 pagesOctober 2017 Ed Infant Fever 29-60 DaysAbdi KebedeNo ratings yet
- Cat Breeding Program: Standard Operating Procedure #624Document3 pagesCat Breeding Program: Standard Operating Procedure #624UrchNo ratings yet
- Congenital SyphilisDocument3 pagesCongenital SyphiliscmvasquezmNo ratings yet
- Abvd Hem HLDocument10 pagesAbvd Hem HLMohammed HaiderNo ratings yet
- Febrile Neonate Clinical Practice Guideline: CatheterizedDocument1 pageFebrile Neonate Clinical Practice Guideline: Catheterizedromeoenny4154No ratings yet
- PCAP ReportDocument28 pagesPCAP ReportAngeline Zamoras-ToledoNo ratings yet
- GilenyaDecember 15 2020Document7 pagesGilenyaDecember 15 2020aishwarya desaiNo ratings yet
- KK Miri MCH Notes Edited March 2017: Compiled by Jody, Fatimah, Wong WM, For KK MiriDocument36 pagesKK Miri MCH Notes Edited March 2017: Compiled by Jody, Fatimah, Wong WM, For KK Mirilailatul husnaNo ratings yet
- 2017 AAP Guidelines For Childhood HypertensionDocument45 pages2017 AAP Guidelines For Childhood HypertensionAulya ArchuletaNo ratings yet
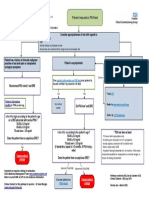
- PSA Pathway: Patient Requests A PSA TestDocument1 pagePSA Pathway: Patient Requests A PSA Testaveen rasulNo ratings yet
- Ob OsceDocument13 pagesOb OsceMark Lopez100% (3)
- CS AlgorithmDocument1 pageCS AlgorithmDraalexNo ratings yet
- Acute PancreatitisDocument11 pagesAcute PancreatitisJessa MaeNo ratings yet
- OBGYN0522 Core ObstetricsDocument5 pagesOBGYN0522 Core ObstetricsSMA N 1 TOROHNo ratings yet
- Cleft Lip or PalateDocument19 pagesCleft Lip or PalateAnonymous LCLG7siTYnNo ratings yet
- Rivalta TestDocument1 pageRivalta TestAmarnath MuthukrishnanNo ratings yet
- Namibia Flipchart Algorithm Child Sep2010Document11 pagesNamibia Flipchart Algorithm Child Sep2010Gabriela Morante RuizNo ratings yet
- Obstetrics & GynaecologyDocument19 pagesObstetrics & GynaecologydrshekarforyouNo ratings yet
- Ya, Dijelaskan Pada Bagian Metode Di StudyDocument4 pagesYa, Dijelaskan Pada Bagian Metode Di StudySepta AryaniNo ratings yet
- Guidelines Colposcopy and Pap Smear Triage GuidelinesDocument12 pagesGuidelines Colposcopy and Pap Smear Triage Guidelinesbabarpdu100% (1)
- SyphilisDocument5 pagesSyphilisNoctrhune AngelNo ratings yet
- Waqas Ahmed Usmani ROLL NO 17-78Document41 pagesWaqas Ahmed Usmani ROLL NO 17-78Waqas Ahmed UsmaniNo ratings yet
- Fluctuaciones Relacionadas A Tratamiento GBDocument7 pagesFluctuaciones Relacionadas A Tratamiento GBOsvaldo CortésNo ratings yet
- Algorithm B Objective Tests For Asthma in Children and Young People Aged 5 To 16 PDF 4656176750Document1 pageAlgorithm B Objective Tests For Asthma in Children and Young People Aged 5 To 16 PDF 4656176750Hakije LakherNo ratings yet
- Management For PROMDocument2 pagesManagement For PROMSajaratul Syifaa'No ratings yet
- Low Dose of CarbamazepineDocument4 pagesLow Dose of CarbamazepineFrank' MeriñoNo ratings yet
- HPV Testing in The Follow-Up of Women Post Colposcopy Treatment - Final VersionDocument16 pagesHPV Testing in The Follow-Up of Women Post Colposcopy Treatment - Final VersionPaulo César López BarrientosNo ratings yet
- Pprom ProtocolDocument3 pagesPprom ProtocolLana kamalNo ratings yet
- WarfarinDocument3 pagesWarfarinJustine CastilloNo ratings yet
- OBSTETRIC HAEMORRHAGE BUNDLES GuidelineDocument8 pagesOBSTETRIC HAEMORRHAGE BUNDLES GuidelineHerwinda GeraldineNo ratings yet
- Validation of Lam Assessment of Employment Readiness (C-LASER) For Chinese Injured WorkersDocument10 pagesValidation of Lam Assessment of Employment Readiness (C-LASER) For Chinese Injured Workerssmartie_chaiNo ratings yet
- Assessing Readiness To Work From A Stages of Change Perspective: Implications For Return To WorkDocument12 pagesAssessing Readiness To Work From A Stages of Change Perspective: Implications For Return To Worksmartie_chaiNo ratings yet
- BLS ExamDocument9 pagesBLS ExamEdwin Delos Reyes Abu100% (3)
- Free First Breakthrough Cryptocurrency Mining Using Phone - "Pi Network App" (Next Bitcoin) (Golden Opportunity To Be Pioneer For Cryptocurrency To Become Rich, Multi-Millionaire and Financial Free)Document2 pagesFree First Breakthrough Cryptocurrency Mining Using Phone - "Pi Network App" (Next Bitcoin) (Golden Opportunity To Be Pioneer For Cryptocurrency To Become Rich, Multi-Millionaire and Financial Free)smartie_chaiNo ratings yet
- Validation of Lam Assessment of Employment Readiness (C-LASER) For Chinese Injured WorkersDocument10 pagesValidation of Lam Assessment of Employment Readiness (C-LASER) For Chinese Injured Workerssmartie_chaiNo ratings yet
- Assessing Readiness To Work From A Stages of Change Perspective: Implications For Return To WorkDocument12 pagesAssessing Readiness To Work From A Stages of Change Perspective: Implications For Return To Worksmartie_chaiNo ratings yet
- Stoke Fall PrecautionDocument31 pagesStoke Fall Precautionsmartie_chai100% (1)
- Elaine Owen - Prosthetic International 254.fullDocument17 pagesElaine Owen - Prosthetic International 254.fullsmartie_chaiNo ratings yet
- Predictor of Post Stroke SpasticityDocument8 pagesPredictor of Post Stroke Spasticitysmartie_chaiNo ratings yet
- Barthel IndexDocument2 pagesBarthel Indexgania100% (1)
- Elaine Owen - Prosthetic International 254.fullDocument17 pagesElaine Owen - Prosthetic International 254.fullsmartie_chaiNo ratings yet
- 2010 Spasticity MechanismsDocument10 pages2010 Spasticity Mechanismsachsyaf arfanNo ratings yet
- SeizureDocument11 pagesSeizuresmartie_chai100% (1)
- Rehab Goal Setting SMARTDocument5 pagesRehab Goal Setting SMARTsmartie_chaiNo ratings yet
- The 2015 BLS ACLS Guidelines ENA PDFDocument36 pagesThe 2015 BLS ACLS Guidelines ENA PDFsmartie_chaiNo ratings yet
- Aequanimitas Tribute To TJ DanarajDocument181 pagesAequanimitas Tribute To TJ DanarajchuhuaNo ratings yet
- Updated 10-16-14 Quick Reference Guide Digital Npuap Epuap Pppia 16oct2014Document75 pagesUpdated 10-16-14 Quick Reference Guide Digital Npuap Epuap Pppia 16oct2014Anonymous kZQet6QA100% (1)
- Good Muscle For Gait Cycle Podiatric - GAIT - ANAL PDFDocument20 pagesGood Muscle For Gait Cycle Podiatric - GAIT - ANAL PDFsmartie_chaiNo ratings yet
- Range of Joint Motion Evaluation Chart OK PDFDocument2 pagesRange of Joint Motion Evaluation Chart OK PDFcesamav100% (4)
- Anatomy of The LegDocument57 pagesAnatomy of The Legsmartie_chaiNo ratings yet
- 2015 ACLS Guideline Update InfographicDocument1 page2015 ACLS Guideline Update Infographiccmalpicac1No ratings yet
- Kinesio CKTT BrochureDocument1 pageKinesio CKTT Brochuresmartie_chaiNo ratings yet
- Pain ModulationDocument10 pagesPain Modulationsmartie_chaiNo ratings yet
- Special Tests LeDocument9 pagesSpecial Tests Lenurasyikah0% (1)
- CPG Management of Type 2 Diabetes Mellitus (5th Edition) Special AFES Congress EditionDocument141 pagesCPG Management of Type 2 Diabetes Mellitus (5th Edition) Special AFES Congress Editionkhangsiean89100% (1)
- 4th Edition of Clinical Practice Guidelines Management of Dyslipidemia 2011Document88 pages4th Edition of Clinical Practice Guidelines Management of Dyslipidemia 2011Farah Aishah HamdanNo ratings yet
- Stroke in PregnancyDocument24 pagesStroke in Pregnancysmartie_chaiNo ratings yet
- Key Sensory PointsDocument6 pagesKey Sensory PointsJose Maria Dominguez RoldanNo ratings yet
- Range of Joint Motion Evaluation Chart OK PDFDocument2 pagesRange of Joint Motion Evaluation Chart OK PDFcesamav100% (4)
- Basic Accounting-PartnerDocument13 pagesBasic Accounting-PartnerSala SahariNo ratings yet
- 10.MIL 9. Current and Future Trends in Media and InformationDocument26 pages10.MIL 9. Current and Future Trends in Media and InformationJonar Marie100% (1)
- CT, PT, IVT, Current Transformer, Potential Transformer, Distribution Boxes, LT Distribution BoxesDocument2 pagesCT, PT, IVT, Current Transformer, Potential Transformer, Distribution Boxes, LT Distribution BoxesSharafatNo ratings yet
- Spring 2021 NBME BreakdownDocument47 pagesSpring 2021 NBME BreakdownUmaNo ratings yet
- Skans Schools of Accountancy CAF-8: Product Units RsDocument2 pagesSkans Schools of Accountancy CAF-8: Product Units RsmaryNo ratings yet
- Bible QuizDocument4 pagesBible QuizjesukarunakaranNo ratings yet
- Literature Is An Important Component of A Total Language Arts Program at All Grade Levels Because of The Many Benefits It OffersDocument1 pageLiterature Is An Important Component of A Total Language Arts Program at All Grade Levels Because of The Many Benefits It Offersbersam05No ratings yet
- Molecular Docking Terhadap Senyawa Kurkumin Dan Arturmeron Pada Tumbuhan Kunyit (Curcuma Longa Linn.) Yang Berpotensi Menghambat Virus CoronaDocument7 pagesMolecular Docking Terhadap Senyawa Kurkumin Dan Arturmeron Pada Tumbuhan Kunyit (Curcuma Longa Linn.) Yang Berpotensi Menghambat Virus Coronalalu reza rezki muanggaraNo ratings yet
- Gucci MurderDocument13 pagesGucci MurderPatsy StoneNo ratings yet
- Aristotle Metaphysics Book V-Delta SachsDocument10 pagesAristotle Metaphysics Book V-Delta Sachsvmishka100% (1)
- Iris Sofía Tobar Quilachamín - Classwork - 16-09-2022Document4 pagesIris Sofía Tobar Quilachamín - Classwork - 16-09-2022IRIS SOFIA TOBAR QUILACHAMINNo ratings yet
- Chapter 4 TeethDocument17 pagesChapter 4 TeethAbegail RuizNo ratings yet
- Bulk Materail International March April 2011 20110300 - 36598714Document20 pagesBulk Materail International March April 2011 20110300 - 36598714ookyilwin3795No ratings yet
- PRTC Tax Final Preboard May 2018Document13 pagesPRTC Tax Final Preboard May 2018BonDocEldRicNo ratings yet
- Solution pdf-51Document68 pagesSolution pdf-51Tanmay GoyalNo ratings yet
- Katyusha Rocket LauncherDocument7 pagesKatyusha Rocket LauncherTepeRudeboyNo ratings yet
- Span of ControlDocument8 pagesSpan of Controlnaveen_gwl100% (4)
- Lynker Technologies LLC U.S. Caribbean Watershed Restoration and Monitoring Coordinator - SE US Job in Remote - GlassdoorDocument4 pagesLynker Technologies LLC U.S. Caribbean Watershed Restoration and Monitoring Coordinator - SE US Job in Remote - GlassdoorCORALationsNo ratings yet
- Gravity & MagneticDocument13 pagesGravity & MagneticBunny Leal100% (1)
- Hallux Valgus SXDocument569 pagesHallux Valgus SXandi100% (2)
- Menken & Sanchez (2020) - Translanguaging in English-Only SchoolsDocument27 pagesMenken & Sanchez (2020) - Translanguaging in English-Only SchoolsSumirah XiaomiNo ratings yet
- Project ProposalDocument1 pageProject ProposalLadee ClaveriaNo ratings yet
- PARAPHRASEDocument19 pagesPARAPHRASETech HelperNo ratings yet
- Timeline of Jewish HistoryDocument33 pagesTimeline of Jewish Historyfabrignani@yahoo.com100% (1)
- Tax Compliance, Moral..Document52 pagesTax Compliance, Moral..PutriNo ratings yet
- Max3080 Max3089Document21 pagesMax3080 Max3089Peter BirdNo ratings yet
- Beginner Guide To Drawing AnimeDocument14 pagesBeginner Guide To Drawing AnimeCharles Lacuna75% (4)
- Assessment Guidelines For Processing Operations Hydrocarbons VQDocument47 pagesAssessment Guidelines For Processing Operations Hydrocarbons VQMatthewNo ratings yet
- Lista Destinatari Tema IDocument4 pagesLista Destinatari Tema INicola IlieNo ratings yet
- OS W2020 3140702 APY MaterialDocument2 pagesOS W2020 3140702 APY MaterialPrince PatelNo ratings yet