You might also like
- Seminar Cs 15 NovDocument24 pagesSeminar Cs 15 Novzeenatn1995No ratings yet
- 1 - Anatomy of KidneysDocument22 pages1 - Anatomy of KidneysAHMAD YUNUSA GARBANo ratings yet
- Kidney: PDF Generated At: Sun, 26 Jan 2014 03:55:26 UTCDocument15 pagesKidney: PDF Generated At: Sun, 26 Jan 2014 03:55:26 UTCVijay RajendiranNo ratings yet
- Renal&Urinary System 2012Document64 pagesRenal&Urinary System 2012Meilani PutriNo ratings yet
- 1 - Anatomy of The KidneyDocument15 pages1 - Anatomy of The Kidneysara khanNo ratings yet
- The KidneysDocument11 pagesThe KidneysJordan MosesNo ratings yet
- Anatomy, Abdomen and Pelvis, Kidneys: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2022 JanDocument6 pagesAnatomy, Abdomen and Pelvis, Kidneys: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2022 Janvenus ohNo ratings yet
- KidneysDocument6 pagesKidneysAmbg GhalyNo ratings yet
- Anatomical Study of The Horseshoe Kidney: Case ReportDocument4 pagesAnatomical Study of The Horseshoe Kidney: Case ReportAndi Raodah ImranNo ratings yet
- Excretory SystemDocument117 pagesExcretory SystemRanjana Das BhowmickNo ratings yet
- Anatomy of Urinary Tract BaruDocument68 pagesAnatomy of Urinary Tract BaruAdya ArradikhaNo ratings yet
- Introduction to the Renal System and Kidney Anatomy (39Document10 pagesIntroduction to the Renal System and Kidney Anatomy (39Jeeson MichaelNo ratings yet
- Anatomy of The Kidney and Ureter: Basic ScienceDocument6 pagesAnatomy of The Kidney and Ureter: Basic ScienceAsfahani LatiefahNo ratings yet
- Kidneys and Urinary Systems ExplainedDocument40 pagesKidneys and Urinary Systems ExplainedOlaifa victorNo ratings yet
- Overview of The Urinary System: N N N NDocument6 pagesOverview of The Urinary System: N N N NDhiyah AuroraNo ratings yet
- Urinary System: Nurmila Sari Anatomi FKIK UIN Syarif Hidayatullah JakartaDocument44 pagesUrinary System: Nurmila Sari Anatomi FKIK UIN Syarif Hidayatullah JakartaSeptiara IqraNo ratings yet
- The Anatomy, Histology and Development of The Kidney PDFDocument14 pagesThe Anatomy, Histology and Development of The Kidney PDFredderdatNo ratings yet
- N Ephron 1111Document9 pagesN Ephron 1111Syed Sakline HossainNo ratings yet
- UNIT 10 (Urinary System)Document6 pagesUNIT 10 (Urinary System)Workinesh Kaynabo KambaloNo ratings yet
- Urinary SystemDocument42 pagesUrinary SystemJose SirittNo ratings yet
- A12SF2 DR QuestionsDocument12 pagesA12SF2 DR QuestionsZafira AkramNo ratings yet
- Anatomy of The Kidney and UreterDocument6 pagesAnatomy of The Kidney and UreterMario Ivan De la Cruz LaraNo ratings yet
- Human Anatomy,: Renal /urinary SystemDocument62 pagesHuman Anatomy,: Renal /urinary Systemsapana shresthaNo ratings yet
- The Kidneys IDocument8 pagesThe Kidneys Ior1da2sa3No ratings yet
- DR Laxman Khanal Bpkihs 07-06-2013Document86 pagesDR Laxman Khanal Bpkihs 07-06-2013Bilal YimamNo ratings yet
- Renal Anatomy and PhysiologyDocument51 pagesRenal Anatomy and PhysiologyAn Zheng100% (3)
- Renal Anatomy and PhysiologyDocument15 pagesRenal Anatomy and PhysiologySapna JainNo ratings yet
- L1 - KidneyDocument27 pagesL1 - KidneyKhadeja JayashNo ratings yet
- MIRADOR, Kiana AnaphyAct16Document4 pagesMIRADOR, Kiana AnaphyAct16Kiana MiradorNo ratings yet
- Ran Ii-Urinary System - 123718Document16 pagesRan Ii-Urinary System - 123718joykibaki066No ratings yet
- Laboratory - Urinary Anatomy - 3Document8 pagesLaboratory - Urinary Anatomy - 3Roisatul MunawarohNo ratings yet
- Kidney AnatomyDocument55 pagesKidney AnatomyMohammad zreadNo ratings yet
- Abdomen OrganDocument64 pagesAbdomen Organriyazadsumaiyajb2003No ratings yet
- Kidney - WikipediaDocument122 pagesKidney - WikipediaMuhammad HuzaifaNo ratings yet
- AIPGMEE 2011 Question Paper With Answers PDFDocument32 pagesAIPGMEE 2011 Question Paper With Answers PDFgayathri67% (3)
- Urinary Sytem - Gross Anatomy Jan 2023Document153 pagesUrinary Sytem - Gross Anatomy Jan 2023bschaliyath.mnlNo ratings yet
- Basic Human Anatomy: Lesson 8: Urogenital SystemDocument19 pagesBasic Human Anatomy: Lesson 8: Urogenital SystemIshita SinghNo ratings yet
- Anatomy Ginjal 2Document16 pagesAnatomy Ginjal 2agung neutronNo ratings yet
- Sys RénalDocument25 pagesSys RénalGregory GebertNo ratings yet
- Prepared by ShakirullahDocument99 pagesPrepared by ShakirullahKhan AbubakarNo ratings yet
- Anatomia RiñonDocument6 pagesAnatomia RiñonJeaneth LanzNo ratings yet
- Human Anatomy & Physiology 243 Unit 2: Urinary & Respiratory System Study GuideDocument5 pagesHuman Anatomy & Physiology 243 Unit 2: Urinary & Respiratory System Study GuideLisetteNo ratings yet
- Anatomy and Physiology-KIDNEYSDocument5 pagesAnatomy and Physiology-KIDNEYSnessie dianne c. cuevasNo ratings yet
- Anatomia UrogenitalDocument8 pagesAnatomia Urogenitalaye97rojasNo ratings yet
- Renal Physiology: The Functions and Anatomy of the KidneysDocument88 pagesRenal Physiology: The Functions and Anatomy of the Kidneysfentaw melkieNo ratings yet
- Location and External Anatomy of The KidneysDocument15 pagesLocation and External Anatomy of The KidneysKyla Malapit GarvidaNo ratings yet
- Chronic Kidney DiseaseDocument25 pagesChronic Kidney DiseaseZachary CohenNo ratings yet
- Kidney and Ureter: L.R. AronsonDocument22 pagesKidney and Ureter: L.R. AronsonDiana GranadaNo ratings yet
- Abiola Seminar in SpleenDocument23 pagesAbiola Seminar in SpleenBamgbose OpeyemiNo ratings yet
- ANPH M3 CU11. Urinary SystemDocument13 pagesANPH M3 CU11. Urinary Systemmia LoremiaNo ratings yet
- Pancreas Organ Functions Blood Sugar Regulation DigestionDocument14 pagesPancreas Organ Functions Blood Sugar Regulation DigestionElena IacobNo ratings yet
- Clinical Oriented Anatomy of Urinary SystemDocument81 pagesClinical Oriented Anatomy of Urinary SystemRizcky Naldy Eka Putra100% (1)
- Chapter I-V-1-Anatomy-Dr-Mark-MakaryDocument17 pagesChapter I-V-1-Anatomy-Dr-Mark-MakaryMark MakaryNo ratings yet
- Bab II Referat BSKDocument26 pagesBab II Referat BSKSandara ParkNo ratings yet
- Chapter 16-Urinary SystemDocument24 pagesChapter 16-Urinary SystemSekar ArumNo ratings yet
- Nephrologi: - PWM Olly Indrajani - 18-3-2015Document128 pagesNephrologi: - PWM Olly Indrajani - 18-3-2015NandatholoeNo ratings yet
- Surgical Anatomy and Anatomical Surgery of The LiverDocument7 pagesSurgical Anatomy and Anatomical Surgery of The LiverAna-Maria MihalceaNo ratings yet
- PPT@Renal System4PC (2022)Document88 pagesPPT@Renal System4PC (2022)ademabdella38No ratings yet
- URS SummaryDocument26 pagesURS SummaryMohamed HaridyNo ratings yet
- Pi Is 0363502313014159Document9 pagesPi Is 0363502313014159Muchamad Wisuda RiswantoNo ratings yet
- Zhu 2017Document3 pagesZhu 2017Muchamad Wisuda RiswantoNo ratings yet
- PolydactylyDocument43 pagesPolydactylyWara Samsarga GedeNo ratings yet
- Level KompetensiDocument7 pagesLevel KompetensiMuchamad Wisuda RiswantoNo ratings yet
- IFU - R910 e CREA - JAFFE 14Document3 pagesIFU - R910 e CREA - JAFFE 14HaisNo ratings yet
- Nephrology ExamsDocument30 pagesNephrology Examsdhianne_garcia2001100% (1)
- Ug NotesDocument538 pagesUg NotesSteven IStudy SmithNo ratings yet
- Aua 2012Document90 pagesAua 2012Tawfiq El-Far100% (5)
- Carolina TrialDocument59 pagesCarolina TrialDr. Abhas ShahNo ratings yet
- Carbuncle, Incision, Drainage, DebridementDocument11 pagesCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinNo ratings yet
- CKD Management HandbookDocument3 pagesCKD Management HandbookMarianaPimentaPinheiroNo ratings yet
- Renal Failure PamphletDocument2 pagesRenal Failure Pamphletapi-236094936No ratings yet
- Katzung QuestionsDocument29 pagesKatzung QuestionsToastie3100% (12)
- Fluconazole Injection, USP: in INTRAVIA Plastic ContainerDocument4 pagesFluconazole Injection, USP: in INTRAVIA Plastic ContainerAnis ThohirohNo ratings yet
- Flucil: Product InformationDocument7 pagesFlucil: Product InformationaaNo ratings yet
- Urinary Tract Infection in Children (National Collaborating Centre For Women's and Children's Health)Document178 pagesUrinary Tract Infection in Children (National Collaborating Centre For Women's and Children's Health)cateterdoblejotaNo ratings yet
- Acute Renal FailureDocument1 pageAcute Renal FailureSonia Letran Singson100% (1)
- Cardiac Biomarkers Expert Advice For CliniciansDocument255 pagesCardiac Biomarkers Expert Advice For CliniciansS Ram KishoreNo ratings yet
- Patho PreeclampsiaDocument7 pagesPatho PreeclampsiaEliza SermoniaNo ratings yet
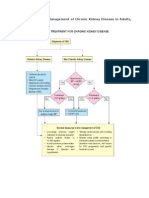
- Summary of CPG Management of CKD in AdultsDocument12 pagesSummary of CPG Management of CKD in AdultsAhmad Zhafri Md NoorNo ratings yet
- 38054 台北市聯合醫院抗生素商品名對照表 PDFDocument99 pages38054 台北市聯合醫院抗生素商品名對照表 PDFka timNo ratings yet
- Medical School PharmDocument187 pagesMedical School PharmSana Savana Aman R100% (1)
- Nephrogenic Systemic Fibrosis: More Questions and Some AnswersDocument9 pagesNephrogenic Systemic Fibrosis: More Questions and Some AnswersJuan MuroNo ratings yet
- Breast CancerDocument108 pagesBreast Cancernasibdin100% (1)
- Hydration in Infants and Children: Vanessa ShawDocument35 pagesHydration in Infants and Children: Vanessa ShawDonya GholamiNo ratings yet
- Diagnosis and treatment of hepatorenal syndromeDocument19 pagesDiagnosis and treatment of hepatorenal syndromeOmar1895No ratings yet
- 10 Polypharmacy Overview and PrinciplesDocument65 pages10 Polypharmacy Overview and PrinciplesNnay Anggraeni100% (1)
- Pregnancy CKD SLIDES EditDocument38 pagesPregnancy CKD SLIDES EditcrsscribdNo ratings yet
- KDIGO AKI Guideline PDFDocument141 pagesKDIGO AKI Guideline PDFAbigail LucasNo ratings yet
- Basic Concepts of Fluid and Electrolyte TherapyDocument136 pagesBasic Concepts of Fluid and Electrolyte Therapymuhammad ajiNo ratings yet
- Case StudyDocument38 pagesCase StudyNissie DegulacionNo ratings yet
- Chronic Kidney DiseaseDocument13 pagesChronic Kidney DiseaseJobelle AcenaNo ratings yet
- AstronautDocument11 pagesAstronautFlorescu VladimirNo ratings yet
- Does The UNOS Heart Transplant Allocation System Favor Men Over Women?Document9 pagesDoes The UNOS Heart Transplant Allocation System Favor Men Over Women?Thumper KatesNo ratings yet