You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Critical Appraisal: The Effect of Ketamine On Hypoventilation During Deep Sedation With Midazolam and PropofolDocument33 pagesCritical Appraisal: The Effect of Ketamine On Hypoventilation During Deep Sedation With Midazolam and PropofolgoldenNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Critical Appraisal PramDocument9 pagesCritical Appraisal PramgoldenNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Hideyuki Higuchi, M.D., Shunichi Takagi, M.D., Kan Zhang, M.D., Ikue Furui, M.D., Makoto Ozaki, M.DDocument6 pagesHideyuki Higuchi, M.D., Shunichi Takagi, M.D., Kan Zhang, M.D., Ikue Furui, M.D., Makoto Ozaki, M.DgoldenNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Universitas Indonesia: U. Weber, M. Krammel, S. Linke, T. Hamp, T. Stimpfl, B. Reiter, W. PlӧchlDocument8 pagesUniversitas Indonesia: U. Weber, M. Krammel, S. Linke, T. Hamp, T. Stimpfl, B. Reiter, W. PlӧchlgoldenNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Ectopic PregnancyDocument26 pagesEctopic PregnancysandhyakrishnanNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Web-Based Versus Home-Based Postnatal Psychoeducational Interventions For First-Time Mothers: A Randomised Controlled TrialDocument13 pagesWeb-Based Versus Home-Based Postnatal Psychoeducational Interventions For First-Time Mothers: A Randomised Controlled Trialnur fadhilahNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- GastroenterologyDocument511 pagesGastroenterologyluiperdvrou100% (3)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Historical Review of MidwiferyDocument32 pagesHistorical Review of MidwiferyVinayak SrivastavaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Sliwa Et Al-2010-European Journal of Heart FailureDocument12 pagesSliwa Et Al-2010-European Journal of Heart FailurealfredoibcNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Jurnal Tetes MataDocument6 pagesJurnal Tetes MataSyafiraNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Dexmedetomidine: Its Use in Intensive Care Medicine and AnaesthesiaDocument5 pagesDexmedetomidine: Its Use in Intensive Care Medicine and AnaesthesiaTarachand LalwaniNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Pacemaker ImplantDocument62 pagesPacemaker Implantadins100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- PQCNC AIM RPC LS3 Ketner Posting 20200303Document41 pagesPQCNC AIM RPC LS3 Ketner Posting 20200303kcochranNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Kinzer Kokich-Managing Congenitally Missing Lateral Incisors Part I Canine Substitution PDFDocument5 pagesKinzer Kokich-Managing Congenitally Missing Lateral Incisors Part I Canine Substitution PDFAdrian Silva SantosNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- PasdfDocument8 pagesPasdfHuy LeNo ratings yet
- CholecystitisDocument12 pagesCholecystitisMariela HuertaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fmge Blue Print PDFDocument1 pageFmge Blue Print PDFLesbputih Gelap100% (1)
- Vascular Surgery OsceDocument66 pagesVascular Surgery Osceapi-19579909233% (3)
- Amnioinfusion - 2Document6 pagesAmnioinfusion - 2Anditha NamiraNo ratings yet
- Hydatidiform MoleDocument2 pagesHydatidiform MolePaola AgustinNo ratings yet
- PheochromocytomaDocument6 pagesPheochromocytomaSonya YuNo ratings yet
- JGCA JPN Classification 3rd EngDocument12 pagesJGCA JPN Classification 3rd EngLiz PesantesNo ratings yet
- Multi-Specialty Hospital: Ram Sharada Healthcare Pvt. LTDDocument48 pagesMulti-Specialty Hospital: Ram Sharada Healthcare Pvt. LTDsubhash goelNo ratings yet
- Eu Directive Annex 5 - List of Qualifications PDFDocument10 pagesEu Directive Annex 5 - List of Qualifications PDFIbrahim ZainabNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- PREMATURIIDocument91 pagesPREMATURIIAdriana MelnicNo ratings yet
- Catheter Care Guidelines PDFDocument45 pagesCatheter Care Guidelines PDFKhaidarni Arni0% (1)
- Procedures in Obstetrics and Gynaecology TextbookDocument272 pagesProcedures in Obstetrics and Gynaecology TextbookPriyaNo ratings yet
- Procedures in O&GDocument7 pagesProcedures in O&GAbdulrahman NajiNo ratings yet
- Scribe ResumeDocument3 pagesScribe ResumetaratoosNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Basic HematologyDocument89 pagesBasic Hematologydrafq2000No ratings yet
- Casestudy Analysis Template Updated 18 Oct 16Document2 pagesCasestudy Analysis Template Updated 18 Oct 16keven319hk4304No ratings yet
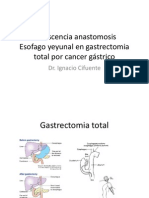
- Dehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástricoDocument22 pagesDehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástriconachooooooooNo ratings yet
- Neonatal ResuscitationDocument15 pagesNeonatal ResuscitationAmruta GadeNo ratings yet
- List of Doctors and Hospitals in Rheinland-PfalzDocument6 pagesList of Doctors and Hospitals in Rheinland-PfalzNamerah AliNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)