You might also like
- Cardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesFrom EverandCardiac Sarcoidosis: Key Concepts in Pathogenesis, Disease Management, and Interesting CasesNo ratings yet
- Efficacy and Safety of Carvedilol in Treatment of Heart Failure With Chronic Kidney DiseaseDocument9 pagesEfficacy and Safety of Carvedilol in Treatment of Heart Failure With Chronic Kidney DiseaseIrma SihotangNo ratings yet
- 2118 FullDocument10 pages2118 FullSergiu NiculitaNo ratings yet
- (Jurnal) Palliative and End-Of-life Care Issues in Chronic Kidney DiseaseDocument10 pages(Jurnal) Palliative and End-Of-life Care Issues in Chronic Kidney DiseaseRizqi DifaNo ratings yet
- Enfermedad Renal CronicaDocument16 pagesEnfermedad Renal CronicaKarina CondeNo ratings yet
- Chronic Kidney Disease: Annals of Internal MedicineDocument16 pagesChronic Kidney Disease: Annals of Internal MedicineJulián Mesa SierraNo ratings yet
- Prevalence and Associated Factors of Frailty and MortalityDocument12 pagesPrevalence and Associated Factors of Frailty and Mortalityor1da2sa3No ratings yet
- Jaha 120 017655Document11 pagesJaha 120 017655Hira SultanNo ratings yet
- Management of Acute Coronary Syndrome in The Older Adult PopulationDocument31 pagesManagement of Acute Coronary Syndrome in The Older Adult PopulationcarramzoNo ratings yet
- Jurnal R2 YerlizaDocument15 pagesJurnal R2 YerlizaYerliza AgrichaNo ratings yet
- Erc PDFDocument16 pagesErc PDFJosé Luis Conde SalazarNo ratings yet
- CCR 15 55 (Recovered 1)Document9 pagesCCR 15 55 (Recovered 1)Raka Petra PrazastaNo ratings yet
- Circoutcomes 117 003665Document6 pagesCircoutcomes 117 003665M EhabNo ratings yet
- SUPER - Recom - Vaccin-ESRD-AJKD-2019Document9 pagesSUPER - Recom - Vaccin-ESRD-AJKD-2019Ioana PanculescuNo ratings yet
- Cardiovascular Complications of Down Syndrome Scoping Review and Expert Consensus PDFDocument17 pagesCardiovascular Complications of Down Syndrome Scoping Review and Expert Consensus PDFDaniela Peinado RiosNo ratings yet
- 2021 IC + Injuria RenalDocument16 pages2021 IC + Injuria RenalAndjela KosticNo ratings yet
- Damluji Et Al 2022 Management of Acute Coronary Syndrome in The Older Adult Population A Scientific Statement From TheDocument31 pagesDamluji Et Al 2022 Management of Acute Coronary Syndrome in The Older Adult Population A Scientific Statement From TheKesia MaldonadoNo ratings yet
- Prevalence of Chronic Kidney Disease in Patients With or at A High Risk of Cardiovascular DiseaseDocument4 pagesPrevalence of Chronic Kidney Disease in Patients With or at A High Risk of Cardiovascular DiseasenuvitaNo ratings yet
- Jaha 121 025205Document32 pagesJaha 121 025205julinka beyla yansonNo ratings yet
- Peripheral Arterial Disease: MBCHB Mres MSC Mrcs Afhea PHDDocument6 pagesPeripheral Arterial Disease: MBCHB Mres MSC Mrcs Afhea PHDNelly ElizabethNo ratings yet
- 01 STR 0000177866 13451 E4Document3 pages01 STR 0000177866 13451 E4Itamar MeirelesNo ratings yet
- Charytan 2017Document9 pagesCharytan 2017Andrew E P SunardiNo ratings yet
- Lai 2021Document10 pagesLai 2021Илија РадосављевићNo ratings yet
- Hypertension Management in Patients With Chronic.7Document7 pagesHypertension Management in Patients With Chronic.7Emillya SariNo ratings yet
- AKI After Cardiac SurgeryDocument9 pagesAKI After Cardiac SurgeryArul KazamaNo ratings yet
- Diabetic RetinopathyDocument11 pagesDiabetic RetinopathyShell PatelNo ratings yet
- Circulationaha 118 037885Document10 pagesCirculationaha 118 037885Mr. TsumNo ratings yet
- Cardiovascular Disease and Its Determinants Public Health IssueDocument5 pagesCardiovascular Disease and Its Determinants Public Health IssueAgus FitrianggaNo ratings yet
- Denby 2017Document11 pagesDenby 2017Marin HarabagiuNo ratings yet
- Jaha 114 001098 PDFDocument18 pagesJaha 114 001098 PDFBerlian NaufalNo ratings yet
- Jurnal Kardio3Document8 pagesJurnal Kardio3Andi SusiloNo ratings yet
- Cafaro 2023 Cardiovascular Risk in Systemic AutDocument2 pagesCafaro 2023 Cardiovascular Risk in Systemic AutSilvia PeresNo ratings yet
- Left Ventricular Diameter and Risk Strati Fication For Sudden Cardiac DeathDocument6 pagesLeft Ventricular Diameter and Risk Strati Fication For Sudden Cardiac DeathKelvin SupriamiNo ratings yet
- Guidline For Stable Coronary Artery DiseaseDocument24 pagesGuidline For Stable Coronary Artery DiseasefitrahtunnisahNo ratings yet
- Cardiovascular Pathophysiology in Chronic Kidney Disease: Opportunities To Transition From Disease To HealthDocument8 pagesCardiovascular Pathophysiology in Chronic Kidney Disease: Opportunities To Transition From Disease To HealthABNo ratings yet
- Anemia: Chronic Kidney DiseaseDocument12 pagesAnemia: Chronic Kidney DiseasetyasNo ratings yet
- Risk Factors For Heart Failure in Patients With Chronic Kidney Disease: The CRIC (Chronic Renal Insuf Ficiency Cohort) StudyDocument10 pagesRisk Factors For Heart Failure in Patients With Chronic Kidney Disease: The CRIC (Chronic Renal Insuf Ficiency Cohort) StudyMarilia Cruz PoloNo ratings yet
- Borman Et Al. 2019 - Survival After End-Stage Renal Failure, Preventing Cardiac Death in ESRDDocument3 pagesBorman Et Al. 2019 - Survival After End-Stage Renal Failure, Preventing Cardiac Death in ESRDShareDialysisNo ratings yet
- Arrhythmia in Cardiac SarcoidosisDocument12 pagesArrhythmia in Cardiac SarcoidosisBinod KumarNo ratings yet
- 1998 Framingham - Prediction Coronary Hearth Disease Using Risk Factor CategoriesDocument12 pages1998 Framingham - Prediction Coronary Hearth Disease Using Risk Factor CategoriesJenny PinillaNo ratings yet
- W-XASIM Issue 5 7A p705 709Document7 pagesW-XASIM Issue 5 7A p705 709chandanNo ratings yet
- Epidemiology and Causes of Chronic Kidney Disease: What's New?Document4 pagesEpidemiology and Causes of Chronic Kidney Disease: What's New?Ika auliaNo ratings yet
- Perioperative Management of Patients With End-Stage Renal DiseaseDocument17 pagesPerioperative Management of Patients With End-Stage Renal DiseaseAn JNo ratings yet
- PIIS0002934321003983Document11 pagesPIIS0002934321003983FinkaNo ratings yet
- JAH3 8 E012030 PDFDocument11 pagesJAH3 8 E012030 PDFmuhammad879No ratings yet
- Chapter 4 Other Complications of CKD CVD Medication Dosa 2013 Kidney InteDocument21 pagesChapter 4 Other Complications of CKD CVD Medication Dosa 2013 Kidney IntewardaninurindahNo ratings yet
- Challenges of Chronic Kidney Disease PreventionDocument3 pagesChallenges of Chronic Kidney Disease PreventionIndah SsntNo ratings yet
- Effects of Statins On Renal FunctionDocument10 pagesEffects of Statins On Renal Functionangela gagariNo ratings yet
- J of Clinical Ultrasound - 2022 - Prastaro - Cardiorenal Syndrome Pathophysiology As A Key To The Therapeutic Approach inDocument15 pagesJ of Clinical Ultrasound - 2022 - Prastaro - Cardiorenal Syndrome Pathophysiology As A Key To The Therapeutic Approach inAkasuna No KujyouNo ratings yet
- Diabetes For Cardiologists Practical Issues in Diagnosis and ManagementDocument12 pagesDiabetes For Cardiologists Practical Issues in Diagnosis and ManagementLuis Alberto OrtizNo ratings yet
- CKD5 HDDocument10 pagesCKD5 HDsari murnaniNo ratings yet
- Psoriasis With Vascular DiseaseDocument4 pagesPsoriasis With Vascular Diseasemegh dutNo ratings yet
- 998 FullDocument7 pages998 FullsilviaNo ratings yet
- Disease Location Is Associated With Survival in Patients With Peripheral Arterial DiseaseDocument23 pagesDisease Location Is Associated With Survival in Patients With Peripheral Arterial DiseaseEvalia ArifinNo ratings yet
- Circoutcomes 119 006260Document9 pagesCircoutcomes 119 006260Anonymous oQtve4oNo ratings yet
- Infecã Ã o e Doenã A CV JACCDocument10 pagesInfecã Ã o e Doenã A CV JACCgpxwdfbqfdNo ratings yet
- Acute Coronary Syndromes CompendiumDocument17 pagesAcute Coronary Syndromes CompendiumInasNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument2 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Jurnal PADDocument8 pagesJurnal PADDiah Rachmania ThalibNo ratings yet
- Referensi Tesis 1Document6 pagesReferensi Tesis 1Endy SusenoNo ratings yet
- Pregnant Woman PowerPoint Templates StandardDocument3 pagesPregnant Woman PowerPoint Templates StandardSriMathi Kasi Malini ArmugamNo ratings yet
- Recovery Room Nurses' Knowledge Regarding Postoperative Airway Emergencies in Adults in Private Hospitals in Northern Gauteng, South AfricaDocument5 pagesRecovery Room Nurses' Knowledge Regarding Postoperative Airway Emergencies in Adults in Private Hospitals in Northern Gauteng, South AfricaSriMathi Kasi Malini ArmugamNo ratings yet
- Teamwork Improvement in Emergency Trauma Departments: Iranian Journal of Nursing and Midwifery Research March 2013Document8 pagesTeamwork Improvement in Emergency Trauma Departments: Iranian Journal of Nursing and Midwifery Research March 2013SriMathi Kasi Malini ArmugamNo ratings yet
- Should Family Be Presence During Resusci PDFDocument3 pagesShould Family Be Presence During Resusci PDFSriMathi Kasi Malini ArmugamNo ratings yet
- Section 3: Post-Operative Care: Edited by DR Justin PhillipsDocument23 pagesSection 3: Post-Operative Care: Edited by DR Justin PhillipsSriMathi Kasi Malini ArmugamNo ratings yet
- Psychological Effects On Patient's Relatives Regarding Their Presence During ResuscitationDocument5 pagesPsychological Effects On Patient's Relatives Regarding Their Presence During ResuscitationSriMathi Kasi Malini ArmugamNo ratings yet
- AphDocument3 pagesAphSriMathi Kasi Malini ArmugamNo ratings yet
- Literature Review Demographics of The End-Stage Renal Disease PopulationDocument22 pagesLiterature Review Demographics of The End-Stage Renal Disease PopulationSriMathi Kasi Malini ArmugamNo ratings yet
- An Uncommon Cause of Antepartum Haemorrhage: A Case Study: January 2019Document7 pagesAn Uncommon Cause of Antepartum Haemorrhage: A Case Study: January 2019SriMathi Kasi Malini ArmugamNo ratings yet
- Can Respir J2015 OczkowskiDocument6 pagesCan Respir J2015 OczkowskiSriMathi Kasi Malini ArmugamNo ratings yet
- Teckhcoff CatheterDocument6 pagesTeckhcoff CatheterSriMathi Kasi Malini ArmugamNo ratings yet
- Admsci 07 00017Document13 pagesAdmsci 07 00017SriMathi Kasi Malini ArmugamNo ratings yet
- Journal Pone 0160541Document8 pagesJournal Pone 0160541SriMathi Kasi Malini ArmugamNo ratings yet
- PP Case Study PsyDocument23 pagesPP Case Study PsySriMathi Kasi Malini ArmugamNo ratings yet
- NIH Public Access: Childhood Maltreatment, Emotional Dysregulation, and Psychiatric ComorbiditiesDocument20 pagesNIH Public Access: Childhood Maltreatment, Emotional Dysregulation, and Psychiatric ComorbiditiesRafael MartinsNo ratings yet
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsDocument2 pagesNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comNo ratings yet
- RRLDocument30 pagesRRLbealinniNo ratings yet
- Article ThymusDocument4 pagesArticle ThymusKima MadNo ratings yet
- APUSH Chapter 1 EssayDocument3 pagesAPUSH Chapter 1 EssayThat DudeNo ratings yet
- Prenatal and Postnatal: DevelopmentDocument22 pagesPrenatal and Postnatal: DevelopmentenergygapNo ratings yet
- Download pdf Bsava Small Animal Formulary 10Th Edition Part A Canine And Feline Fergus Allerton ebook full chapterDocument53 pagesDownload pdf Bsava Small Animal Formulary 10Th Edition Part A Canine And Feline Fergus Allerton ebook full chaptermavis.glover620100% (2)
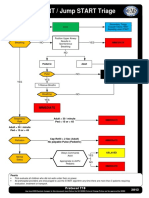
- Start - Jump START Triage PDFDocument2 pagesStart - Jump START Triage PDF081381246529100% (1)
- PostpartumDocument3 pagesPostpartumMuhammad RifaiNo ratings yet
- Proposa DAFPUS Awal Nian NianDocument4 pagesProposa DAFPUS Awal Nian NianAnia RandowichNo ratings yet
- Lesson Plan On Intestinal ObstructionDocument41 pagesLesson Plan On Intestinal ObstructionLoma Waghmare (Jadhav)100% (1)
- Medical Essential Certificate-ADocument2 pagesMedical Essential Certificate-AShahed HusaainNo ratings yet
- 8-1-11 - Pig Heart Dissection - LessonDocument7 pages8-1-11 - Pig Heart Dissection - LessonJoan NicoleNo ratings yet
- Nlenvirte 3082Document8 pagesNlenvirte 3082api-244168124No ratings yet
- Material Safety Data Sheet: A264 Corrosion Inhibitor A264Document9 pagesMaterial Safety Data Sheet: A264 Corrosion Inhibitor A264MasoudTeimooriNo ratings yet
- Epidural NeuroplastyDocument13 pagesEpidural NeuroplastyadityakurniantoNo ratings yet
- Presentation DR Tourville - IGSDocument7 pagesPresentation DR Tourville - IGSadesamboraNo ratings yet
- Regina L. Alfeche / Denise Monikha F. Caballo / Ryan Carlo P. Fajardo / Almera A. Limpao II / Wanesha M. MustaphaDocument10 pagesRegina L. Alfeche / Denise Monikha F. Caballo / Ryan Carlo P. Fajardo / Almera A. Limpao II / Wanesha M. MustaphaGenalin M. Escobia-BagasNo ratings yet
- TCM Internal Medicine Simplified - HandoutDocument94 pagesTCM Internal Medicine Simplified - HandoutSam Gt100% (2)
- Informatics Solution For Emergency Preparedness and ResponseDocument4 pagesInformatics Solution For Emergency Preparedness and ResponseLuisseBeaI.BrazaNo ratings yet
- Overview of Nurses' Role in Management of Patient With Atrial FibrillationDocument5 pagesOverview of Nurses' Role in Management of Patient With Atrial FibrillationAhmed AlkhaqaniNo ratings yet
- F5000 ManualDocument6 pagesF5000 Manualcase1965No ratings yet
- TO Anatomy & PhysiologyDocument67 pagesTO Anatomy & PhysiologyshasheNo ratings yet
- Setting GuideDocument12 pagesSetting GuideJamesNo ratings yet
- Lesson Plan On Theory.Document12 pagesLesson Plan On Theory.Bhumi ChouhanNo ratings yet
- Lesson 4Document3 pagesLesson 4Makilan CharleneNo ratings yet
- CBT 2 QuestionsDocument4 pagesCBT 2 QuestionsDick Morgan Ferrer100% (1)
- Management of COPDDocument480 pagesManagement of COPDjoeyjoe82No ratings yet
- 1111 - Microbiological Examination of Nonsterile Products - Acceptance Criteria For Pharmaceutical Preparations and Substances For Pharmaceutical UseDocument2 pages1111 - Microbiological Examination of Nonsterile Products - Acceptance Criteria For Pharmaceutical Preparations and Substances For Pharmaceutical UseCarolina MontoyaNo ratings yet
- Rhetorical AnalysisDocument7 pagesRhetorical Analysisapi-242615070100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (36)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (4)
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeFrom EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeRating: 4.5 out of 5 stars4.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 4 out of 5 stars4/5 (5)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesFrom EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesRating: 4.5 out of 5 stars4.5/5 (1412)
- I Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionFrom EverandI Shouldn't Feel This Way: Name What’s Hard, Tame Your Guilt, and Transform Self-Sabotage into Brave ActionNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (44)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (170)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (46)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (254)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (267)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Summary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: Thinking, Fast and Slow: by Daniel Kahneman: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (61)