You might also like
- Bashh WartsDocument19 pagesBashh WartsKeeranmayeeishraNo ratings yet
- Guidelines on the Management of Trichomonas vaginalis 2014Document9 pagesGuidelines on the Management of Trichomonas vaginalis 2014Defry Yoga ArtantoNo ratings yet
- Consultas GU de Varones AdolescentesDocument18 pagesConsultas GU de Varones AdolescentessantiagoNo ratings yet
- Molluscum Contagiosum 2014 FinalDocument20 pagesMolluscum Contagiosum 2014 FinalKemal TaufikNo ratings yet
- Hillman R. 2016 - IANS - International - Guidelines - For - Practice.2 PDFDocument9 pagesHillman R. 2016 - IANS - International - Guidelines - For - Practice.2 PDFLaura Cristina Restrepo MéndezNo ratings yet
- Bashh PidDocument26 pagesBashh PidMarNo ratings yet
- 2013 UK National Guideline For The Management of Lymphogranuloma VenereumDocument10 pages2013 UK National Guideline For The Management of Lymphogranuloma VenereumAmelia Dyati PutriNo ratings yet
- HSV Final Guidelines With Ref SortedDocument22 pagesHSV Final Guidelines With Ref SortedScOta Adoncia RaekanafEezaNo ratings yet
- Effective Screening10Document4 pagesEffective Screening10ponekNo ratings yet
- Guideline On The Management of Anogenita WartsDocument9 pagesGuideline On The Management of Anogenita WartsIqra AnugerahNo ratings yet
- Pid 2018Document26 pagesPid 2018Nousen TaraNo ratings yet
- Bacterial VaginosisDocument15 pagesBacterial VaginosisMarcel BejanNo ratings yet
- 2018 UK National Guideline For The Management of Infection With Neisseria GonorrhoeaeDocument12 pages2018 UK National Guideline For The Management of Infection With Neisseria GonorrhoeaeMuneeb ShiekhNo ratings yet
- Mustafa 2016Document7 pagesMustafa 2016ejigsonNo ratings yet
- COVID-19 Testing: A Reflection On Test Accuracy in The Real WorldDocument34 pagesCOVID-19 Testing: A Reflection On Test Accuracy in The Real Worldjoeboots78No ratings yet
- Kondiloma AkuminataDocument4 pagesKondiloma AkuminataIntan PermataNo ratings yet
- Original Article Vaginal Discharge: Perceptions and Health Seeking Behavior Among Nepalese WomenDocument5 pagesOriginal Article Vaginal Discharge: Perceptions and Health Seeking Behavior Among Nepalese WomennovywardanaNo ratings yet
- VPH CancerDocument4 pagesVPH CancerJader Aldair Pavon GomezNo ratings yet
- WHO RHR 08.14 EngDocument14 pagesWHO RHR 08.14 Engkyle31No ratings yet
- An Update On The Management of Endometrial HyperplasiaDocument5 pagesAn Update On The Management of Endometrial Hyperplasiafitrah fajrianiNo ratings yet
- Vaginal Discharge: Clinical ReviewDocument5 pagesVaginal Discharge: Clinical ReviewOktari Dwi YantiNo ratings yet
- Clinical Characteristicsof Mycoplasmagenitaliumandthe Usefulnessof Syndromic Management Among Women Living With Human Immunodeficiency VirusDocument4 pagesClinical Characteristicsof Mycoplasmagenitaliumandthe Usefulnessof Syndromic Management Among Women Living With Human Immunodeficiency VirusThania WazintaNo ratings yet
- HPV Infections: Mucosal Types and Genital WartsDocument6 pagesHPV Infections: Mucosal Types and Genital WartsChristy BradyNo ratings yet
- WHO/BS/06.2050 - Final English Only: Expert Committee On Biological StandardizationDocument66 pagesWHO/BS/06.2050 - Final English Only: Expert Committee On Biological StandardizationSleeping KnightNo ratings yet
- Int J STD Aids 2013 Bignell 85 92Document8 pagesInt J STD Aids 2013 Bignell 85 92Ir Ardy YusriawanNo ratings yet
- Prevalence and Incidence of Genital Warts and Cervical Human Papillomavirus Infections in Nigerian WomenDocument10 pagesPrevalence and Incidence of Genital Warts and Cervical Human Papillomavirus Infections in Nigerian WomenRiszki_03No ratings yet
- Final Compilation - Group D ProjectDocument75 pagesFinal Compilation - Group D ProjectRukaiya Auwal AliNo ratings yet
- TB Research Papers PDFDocument8 pagesTB Research Papers PDFh02rj3ek100% (1)
- All India Institute of Local Self Government Delhi: "National Aids Control ProgrammeDocument18 pagesAll India Institute of Local Self Government Delhi: "National Aids Control ProgrammeMilan NayekNo ratings yet
- Multi-Country Monkeypox Outbreak - Situation UpdateDocument12 pagesMulti-Country Monkeypox Outbreak - Situation UpdateDita Odylia DitaNo ratings yet
- Civ813 PDFDocument7 pagesCiv813 PDFzevillaNo ratings yet
- Gynecology & Reproductive HealthDocument6 pagesGynecology & Reproductive HealthtiaranindyNo ratings yet
- 726 Genital Warts DSTDocument6 pages726 Genital Warts DSTNurul JannahNo ratings yet
- Esmo. Cancer de AnoDocument11 pagesEsmo. Cancer de AnoCarlos Cruz RNo ratings yet
- Anal Cancer - ESMO-ESSO-ESTRO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpDocument11 pagesAnal Cancer - ESMO-ESSO-ESTRO Clinical Practice Guidelines For Diagnosis, Treatment and Follow-UpNasrudin EfendiNo ratings yet
- StdsDocument71 pagesStdsabel semuNo ratings yet
- Aagl Practice Guidelines For The Diagnosis and Management of Endometrial Polyps PDFDocument8 pagesAagl Practice Guidelines For The Diagnosis and Management of Endometrial Polyps PDFhusain abdul halimNo ratings yet
- Tatalaksana Dan Pencegahan - Hal 29-38 - Cancer of The Cervix Uteri 2021 UpdateDocument17 pagesTatalaksana Dan Pencegahan - Hal 29-38 - Cancer of The Cervix Uteri 2021 UpdateAl-Amirah ZainabNo ratings yet
- UK National Guideline For The Management of Pelvic Inflamatory DiseaseDocument18 pagesUK National Guideline For The Management of Pelvic Inflamatory Diseasealejandro perez sanchezNo ratings yet
- Intl J Gynecology Obste - 2021 - BhatlaDocument17 pagesIntl J Gynecology Obste - 2021 - BhatlaKalaivathanan VathananNo ratings yet
- Intl J Gynecology Obste - 2021 - Bhatla - Cancer of The Cervix Uteri 2021 UpdateDocument17 pagesIntl J Gynecology Obste - 2021 - Bhatla - Cancer of The Cervix Uteri 2021 UpdateKim RamirezNo ratings yet
- Prevalence and Incidence of External Genital Warts in A Sample of Italian General Female PopulationDocument8 pagesPrevalence and Incidence of External Genital Warts in A Sample of Italian General Female PopulationArief FerrariNo ratings yet
- RMV 2034Document6 pagesRMV 2034Ga HernandezNo ratings yet
- Rapid On-site Evaluation (ROSE): A Practical GuideFrom EverandRapid On-site Evaluation (ROSE): A Practical GuideGuoping CaiNo ratings yet
- Etiopathogenesis and Natural History of Carcinoma Cervix: Human Papilloma Virus High Risk FactorsDocument33 pagesEtiopathogenesis and Natural History of Carcinoma Cervix: Human Papilloma Virus High Risk FactorsNatasya Ayusandra MahersaputriNo ratings yet
- The Global Epidemiology of Bacterial Vaginosis A Systematic ReviewDocument19 pagesThe Global Epidemiology of Bacterial Vaginosis A Systematic ReviewcheracapNo ratings yet
- Cervical Cancer Literature ReviewDocument6 pagesCervical Cancer Literature Reviewaflskeqjr100% (1)
- Esophageal ulcer case report links HPV infection to cureDocument2 pagesEsophageal ulcer case report links HPV infection to cureTomi EscribanoNo ratings yet
- Health-Care Workers' Occupational Exposures To Body Fluids in 21 Countries in Africa: Systematic Review and Meta-AnalysisDocument17 pagesHealth-Care Workers' Occupational Exposures To Body Fluids in 21 Countries in Africa: Systematic Review and Meta-AnalysisgusdeNo ratings yet
- Prevalence and Associated Factors of HIV Infection Among Pregnant Women Attending Antenatal Care at The Yaoundé Central HospitalDocument6 pagesPrevalence and Associated Factors of HIV Infection Among Pregnant Women Attending Antenatal Care at The Yaoundé Central HospitalnabilahbilqisNo ratings yet
- Cervical Cancer ESMODocument12 pagesCervical Cancer ESMOAndrei CorhaNo ratings yet
- HPV Research Paper TopicDocument8 pagesHPV Research Paper Topicgz8y0esp100% (1)
- Cancer de PeneDocument12 pagesCancer de PeneAndelcass DellNo ratings yet
- Retest Guidelines As Per WHODocument36 pagesRetest Guidelines As Per WHODevendra NiranjanNo ratings yet
- Appropriate, Screening For Sexually Transmitted Infections Every 6 Months For HIV-positive Patients Under Follow-Up. This May Be Within The Clinic Itself or by Referral To Appropriate ColleaguesDocument9 pagesAppropriate, Screening For Sexually Transmitted Infections Every 6 Months For HIV-positive Patients Under Follow-Up. This May Be Within The Clinic Itself or by Referral To Appropriate ColleaguestjiproetNo ratings yet
- Health Technology Assessment On Cervical Cancer Screening 20002014Document10 pagesHealth Technology Assessment On Cervical Cancer Screening 20002014Reni HariyantiNo ratings yet
- Guidelines for managing abnormally invasive placentaDocument16 pagesGuidelines for managing abnormally invasive placentaErika GuerreroNo ratings yet
- Pediatric Cervical Lymphadenopathy GuideDocument11 pagesPediatric Cervical Lymphadenopathy GuideAMENDBENo ratings yet
- Reproductive Health Indicators ExplainedDocument17 pagesReproductive Health Indicators ExplainedRogers Talemwa WakefieldNo ratings yet
- Anomali Uterus PDFDocument13 pagesAnomali Uterus PDFsundariNo ratings yet
- GTG 56 PDFDocument24 pagesGTG 56 PDFKadelsy BristolNo ratings yet
- FIGO Cancer Report 2018 PDFDocument128 pagesFIGO Cancer Report 2018 PDFAndi Tiara S. AdamNo ratings yet
- FIGOCEDocument11 pagesFIGOCEAldwin TanuwijayaNo ratings yet
- STD Treatment 2015Document140 pagesSTD Treatment 2015Supalerk KowinthanaphatNo ratings yet
- STD Treatment 2015Document140 pagesSTD Treatment 2015Supalerk KowinthanaphatNo ratings yet
- The New WHO Classification of Ovarian Fallopian Tu PDFDocument2 pagesThe New WHO Classification of Ovarian Fallopian Tu PDFRahmawati Dianing PangestuNo ratings yet
- Genital Warts & PregnancyDocument24 pagesGenital Warts & PregnancyRahmawati Dianing PangestuNo ratings yet
- External Cephalic VersionDocument14 pagesExternal Cephalic VersionRahmawati Dianing Pangestu100% (1)
- Meng 2013Document8 pagesMeng 2013Rahmawati Dianing PangestuNo ratings yet
- Guide to Breech Presentation DeliveryDocument13 pagesGuide to Breech Presentation DeliveryRahmawati Dianing PangestuNo ratings yet
- Cell Signaling and Second Messaging Tugas DR - Agung SpogDocument8 pagesCell Signaling and Second Messaging Tugas DR - Agung SpogRahmawati Dianing PangestuNo ratings yet
- Espl in 2017Document10 pagesEspl in 2017Rahmawati Dianing PangestuNo ratings yet
- Breech SimulationDocument10 pagesBreech SimulationRahmawati Dianing PangestuNo ratings yet
- Kuliah FisiologiDocument13 pagesKuliah FisiologiRahmawati Dianing PangestuNo ratings yet
- SP-200 Advanced PumpDocument4 pagesSP-200 Advanced PumpOsvaldo BravoNo ratings yet
- Symbol High Low R5 R4 R3 R2: DailyDocument8 pagesSymbol High Low R5 R4 R3 R2: Daily257597 rmp.mech.16No ratings yet
- Factors Affecting Movement of Beta-Lain Pigment in Beetroot CellsDocument3 pagesFactors Affecting Movement of Beta-Lain Pigment in Beetroot Cellszarahirani25% (4)
- Effectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsDocument8 pagesEffectiveness of Breathing Exercise On Reducing Pain Perception and State Anxiety Among Primi ParturientsPutra SpNo ratings yet
- Fingertip Injuries Diagnosis, Management and ReconstructionDocument197 pagesFingertip Injuries Diagnosis, Management and Reconstructionokida192No ratings yet
- Operator Manual For Respons920 With ISE - v2016.02Document358 pagesOperator Manual For Respons920 With ISE - v2016.02Juan Pablo CondoriNo ratings yet
- Work Permit Renewal Application FormDocument2 pagesWork Permit Renewal Application FormyamojodnabNo ratings yet
- GMP TD Ar FPL 11033Document1 pageGMP TD Ar FPL 11033Sammy NguyenNo ratings yet
- Fermentation Technology for Food Preservation and ProcessingDocument47 pagesFermentation Technology for Food Preservation and ProcessingAhmad Syamil Muhamad ZinNo ratings yet
- Agriculture Class-8Document67 pagesAgriculture Class-8Sahej100% (2)
- Chap 24 Econ 40Document4 pagesChap 24 Econ 40Racel DelacruzNo ratings yet
- (IJCST-V11I6P5) :A.E.E. El-Alfi, M. E. A. Awad, F. A. A. KhalilDocument9 pages(IJCST-V11I6P5) :A.E.E. El-Alfi, M. E. A. Awad, F. A. A. KhalilEighthSenseGroupNo ratings yet
- Spares Parts Cannibalisation ProcedureDocument3 pagesSpares Parts Cannibalisation ProcedureThang Nguyen Hung100% (1)
- 3M Bio-Acoustic Simulator User Manual (053-012 Rev D)Document21 pages3M Bio-Acoustic Simulator User Manual (053-012 Rev D)rodrigocornejo81No ratings yet
- Intro To GymnasticsDocument69 pagesIntro To GymnasticsMichaela Celerio50% (2)
- BONDING: Understanding Chemical AttractionsDocument201 pagesBONDING: Understanding Chemical AttractionsKhaled OsmanNo ratings yet
- Detailed Lesson Plan in Household Services Adiel RavaneraDocument8 pagesDetailed Lesson Plan in Household Services Adiel RavaneraAdielNo ratings yet
- Let's Check: To Eliminate Unrealized Gain On Sale of LandDocument4 pagesLet's Check: To Eliminate Unrealized Gain On Sale of Landalmira garciaNo ratings yet
- REMOTE Calculator Tool May 21 2013Document77 pagesREMOTE Calculator Tool May 21 2013Leyner Garcia MezquitaNo ratings yet
- Manoshe Street Takeaway MenuDocument9 pagesManoshe Street Takeaway MenuimaddakrNo ratings yet
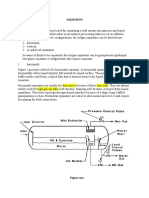
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- 342Mass&HeatModule (3) Soln071118 OlefinPlantDocument12 pages342Mass&HeatModule (3) Soln071118 OlefinPlantmanuelNo ratings yet
- LC Used in ProteimicsDocument15 pagesLC Used in ProteimicsMandu ManNo ratings yet
- Water For Injections BP: What Is in This Leaflet?Document2 pagesWater For Injections BP: What Is in This Leaflet?Mohamed OmerNo ratings yet
- BiostastisticDocument2 pagesBiostastisticاحمد ماجد زبنNo ratings yet
- Hydrostatic Testing ProcedureDocument21 pagesHydrostatic Testing ProcedureFerdie OSNo ratings yet
- English Sds Turalik 52Document13 pagesEnglish Sds Turalik 52Muhammad ArifudinNo ratings yet
- Indian Medical Tourism Industry: A Pathway For The Healthy Future of IndiaDocument13 pagesIndian Medical Tourism Industry: A Pathway For The Healthy Future of IndiaPranjal MaluNo ratings yet
- Information Security Management System: Gheorghe MirelaDocument6 pagesInformation Security Management System: Gheorghe MirelaChristen CastilloNo ratings yet
- Make Every Day Count: George Eliot's inspirational poemDocument3 pagesMake Every Day Count: George Eliot's inspirational poemRUTUJA KALENo ratings yet