You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Mock Trial ScriptDocument25 pagesMock Trial ScriptRonilo Subaan94% (18)
- CPT Coding Practice AnswersDocument17 pagesCPT Coding Practice AnswersTannu SamadNo ratings yet
- Civil Law Compilation Bar Q&a 1990-2017 PDFDocument380 pagesCivil Law Compilation Bar Q&a 1990-2017 PDFReynaldo Yu100% (10)
- The ABCDE ApproachDocument4 pagesThe ABCDE Approachazmar3No ratings yet
- 17-18 Chong Kar Mun's Anaesthesia NotesDocument32 pages17-18 Chong Kar Mun's Anaesthesia NotesElaineNo ratings yet
- GEA ProtocolsDocument101 pagesGEA Protocolsffbrians100% (1)
- Equitable PCI Vs TanDocument2 pagesEquitable PCI Vs TanMosarah AltNo ratings yet
- Equitable PCI Vs TanDocument2 pagesEquitable PCI Vs TanMosarah AltNo ratings yet
- Spec Com BQsDocument15 pagesSpec Com BQsMosarah AltNo ratings yet
- Banking and AMLADocument26 pagesBanking and AMLAMosarah AltNo ratings yet
- AA Course-Difficult Airway1Document54 pagesAA Course-Difficult Airway1Anonymous V5xDcrNo ratings yet
- Tax Case Digests CompilationDocument207 pagesTax Case Digests CompilationFrancis Ray Arbon Filipinas83% (24)
- Tax Case Digests CompilationDocument207 pagesTax Case Digests CompilationFrancis Ray Arbon Filipinas83% (24)
- Metropolitan Bank Vs Wilfred ChiokDocument1 pageMetropolitan Bank Vs Wilfred ChiokMosarah AltNo ratings yet
- Rights of The AccusedDocument13 pagesRights of The AccusedLorebeth EspañaNo ratings yet
- MCQ Anaesthesia QuestionsDocument4 pagesMCQ Anaesthesia Questionsapi-2629165181% (32)
- Lasers in Maxillofacial Surgery and Dentistry 0865775664 PDFDocument168 pagesLasers in Maxillofacial Surgery and Dentistry 0865775664 PDFIrina OneaNo ratings yet
- Illustrated Clinical Cases PDFDocument321 pagesIllustrated Clinical Cases PDFPablo Lukacs Carmona100% (2)
- Update in AnaesthesiaDocument52 pagesUpdate in AnaesthesiaRoy ANo ratings yet
- Salazar Vs JY BrothersDocument4 pagesSalazar Vs JY BrothersMosarah AltNo ratings yet
- CABG PathwayDocument5 pagesCABG PathwayHardyansyah Harisman100% (1)
- Ting Ting Pua V Sps TiongDocument2 pagesTing Ting Pua V Sps TiongeieipayadNo ratings yet
- Abad Vs PhilcomsatDocument2 pagesAbad Vs PhilcomsatFiels GamboaNo ratings yet
- Oxygen TherapyDocument3 pagesOxygen TherapyKristina PingolNo ratings yet
- People V WagasDocument1 pagePeople V WagasMosarah AltNo ratings yet
- Pretrial Process FlowDocument1 pagePretrial Process FlowMosarah AltNo ratings yet
- 2021 Schedule of Preweek LecturesDocument1 page2021 Schedule of Preweek LecturesMarcky MarionNo ratings yet
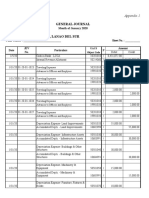
- General Journal: Appendix 1Document5 pagesGeneral Journal: Appendix 1Mosarah AltNo ratings yet
- LectureDocument25 pagesLectureMarieNo ratings yet
- Politicsl LawDocument91 pagesPoliticsl LawMosarah AltNo ratings yet
- Tax DigestsDocument13 pagesTax DigestsMosarah AltNo ratings yet
- San Miguel Corp Vs PuzonDocument2 pagesSan Miguel Corp Vs PuzonMosarah AltNo ratings yet
- Cayanan Vs North StarDocument2 pagesCayanan Vs North StarMosarah AltNo ratings yet
- PNB Vs BalmacedaDocument2 pagesPNB Vs BalmacedaMosarah AltNo ratings yet
- Equitable Banking Vs Special SteelDocument1 pageEquitable Banking Vs Special SteelMosarah AltNo ratings yet
- Politicsl LawDocument91 pagesPoliticsl LawMosarah AltNo ratings yet
- Tax ReviewerDocument45 pagesTax ReviewerMosarah AltNo ratings yet
- Sps Ros Vs PNB 2011 PDFDocument8 pagesSps Ros Vs PNB 2011 PDFMosarah AltNo ratings yet
- Siochi Vs CA 2010 PDFDocument9 pagesSiochi Vs CA 2010 PDFMosarah AltNo ratings yet
- Sps Uy Vs CA 2000Document7 pagesSps Uy Vs CA 2000Mosarah AltNo ratings yet
- Ching Vs CA 1990Document6 pagesChing Vs CA 1990Mosarah AltNo ratings yet
- Cuff Pressure GaugesDocument1 pageCuff Pressure GaugesMatías100% (1)
- 6.paediatric BronchosDocument7 pages6.paediatric BronchosDR K C MALLIKNo ratings yet
- Co2 - Sensor-Kit - p900 - 05 Nihon Kohden BSM 2301 KDocument4 pagesCo2 - Sensor-Kit - p900 - 05 Nihon Kohden BSM 2301 KpabloNo ratings yet
- AnestesiDocument11 pagesAnestesiAnonymous 8w9QEGNo ratings yet
- Information MSQ KROK 2 Medicine 2007 2020 ANESTHESIOLOGYEMERGENCYDocument73 pagesInformation MSQ KROK 2 Medicine 2007 2020 ANESTHESIOLOGYEMERGENCYHikufe JesayaNo ratings yet
- IE Visualisation Platform Brochure 496951001 V01 1113Document7 pagesIE Visualisation Platform Brochure 496951001 V01 1113Eugenio Daniel Martinez HurtadoNo ratings yet
- Post-Operative Fever EditDocument52 pagesPost-Operative Fever EditDebsNo ratings yet
- BASKA MASK & Spinal NeedleDocument32 pagesBASKA MASK & Spinal NeedleAnkush MalhotraNo ratings yet
- Acute Respiratory Distress Syndrome (ARDS)Document85 pagesAcute Respiratory Distress Syndrome (ARDS)Jose Adan Vazquez MoralesNo ratings yet
- Airway AssessmentDocument26 pagesAirway AssessmentShehan WijayasiriwardanaNo ratings yet
- DR Ty BLS PALS1Document4 pagesDR Ty BLS PALS1Burt Robinson LayosNo ratings yet
- Biomedica Manikins CatalogDocument64 pagesBiomedica Manikins CatalogRahul KashyapNo ratings yet
- Golden Hour TraumaDocument5 pagesGolden Hour Traumalevaniah renganathanNo ratings yet
- Worksheet - Respiratory SystemDocument8 pagesWorksheet - Respiratory SystemDhen MarcNo ratings yet
- Singhania University Rajasthan: (Yearly Programme)Document13 pagesSinghania University Rajasthan: (Yearly Programme)om vermaNo ratings yet
- Emcrit Airway Checklist 2013 02 05 PDFDocument3 pagesEmcrit Airway Checklist 2013 02 05 PDFspamvarunNo ratings yet
- Peadiatric Advanced Life Support (Pals)Document18 pagesPeadiatric Advanced Life Support (Pals)SREEDEVI T SURESHNo ratings yet
- Special Needs PopulationDocument13 pagesSpecial Needs PopulationVina EmpialesNo ratings yet
- Effect of Intravenous Oxycodone On The Physiologic Responses To Extubation Following General AnesthesiaDocument6 pagesEffect of Intravenous Oxycodone On The Physiologic Responses To Extubation Following General AnesthesiaYulia Astari SupratmanNo ratings yet