You might also like
- LeucemieDocument2 pagesLeucemieMădălina MoldovanuNo ratings yet
- 6255 24879 1 PBDocument2 pages6255 24879 1 PBSyafatesia nicky pratiwiNo ratings yet
- Ultrasound "Whirlpool Sign" For Midgut Volvulus: Muktachand L. Rokade, Sushila Yamgar, Devesh TawriDocument3 pagesUltrasound "Whirlpool Sign" For Midgut Volvulus: Muktachand L. Rokade, Sushila Yamgar, Devesh TawrizzzNo ratings yet
- The Misplaced Caecum and The Root of The MesenteryDocument8 pagesThe Misplaced Caecum and The Root of The MesenteryKrsna DharmasyaNo ratings yet
- The Changing Spectrum of Intestinal MalrDocument8 pagesThe Changing Spectrum of Intestinal MalrAbelardo tabordaNo ratings yet
- Vascular AccententDocument2 pagesVascular Accententwp4saleNo ratings yet
- Poster MidgutDocument1 pagePoster MidgutMuruga PrakashNo ratings yet
- Bilious Vomiting in The NewbornDocument6 pagesBilious Vomiting in The NewbornRodrigo Vargas IllescasNo ratings yet
- Jurnal 1Document6 pagesJurnal 1rahayuNo ratings yet
- Common Pitfalls in Paediatric Abdominal Imaging: ReviewDocument3 pagesCommon Pitfalls in Paediatric Abdominal Imaging: ReviewMaria JoseNo ratings yet
- AdminDocument5 pagesAdminFirman adiNo ratings yet
- 1 s2.0 S0263931914001124 MainDocument4 pages1 s2.0 S0263931914001124 MainOttofianus Hewick KalangiNo ratings yet
- 5 Congenital Malformation (Continue)Document4 pages5 Congenital Malformation (Continue)Mohamed Al-zichrawyNo ratings yet
- Pemeriksaan Rontgen Toraks, Elektrokardiogram (EKG), USG Abdomen Dan EchocardiografiDocument5 pagesPemeriksaan Rontgen Toraks, Elektrokardiogram (EKG), USG Abdomen Dan EchocardiografigorodoeNo ratings yet
- Sijog 47 291-296Document6 pagesSijog 47 291-296IcicNo ratings yet
- Anorectal MalformationDocument6 pagesAnorectal MalformationMaryam AkmalNo ratings yet
- Vitellointestinal Duct Anomalies in InfancyDocument3 pagesVitellointestinal Duct Anomalies in InfancyRonjavafantillanNo ratings yet
- Cloacal MalformationsDocument6 pagesCloacal MalformationsRayhanun MardhatillahNo ratings yet
- Journal of Rare Diseases MARDocument13 pagesJournal of Rare Diseases MARDaiiny DelgadoNo ratings yet
- Twinpregnancy Bi Chorial Complicatedwithexomphalos of One Twin: Case ReportDocument4 pagesTwinpregnancy Bi Chorial Complicatedwithexomphalos of One Twin: Case ReportIJAR JOURNALNo ratings yet
- Management of The Colonic Volvulus in 2016Document10 pagesManagement of The Colonic Volvulus in 2016alexandraNo ratings yet
- Parurethral CystsDocument3 pagesParurethral CystsIoannis ValioulisNo ratings yet
- JURNAL Volvulus 2-DikonversiDocument16 pagesJURNAL Volvulus 2-DikonversiLucya WulandariNo ratings yet
- Gastroschisis Omphalocele PDFDocument5 pagesGastroschisis Omphalocele PDFFariz Eka SetiawanNo ratings yet
- Sugai, 2008 MRI OmphaloceleDocument3 pagesSugai, 2008 MRI OmphaloceleNurul ArdaniNo ratings yet
- Successful Treatment of A 14-Year-Old Patient With Intestinal Malrotation With Laparoscopic Ladd Procedure: Case Report and Literature ReviewDocument5 pagesSuccessful Treatment of A 14-Year-Old Patient With Intestinal Malrotation With Laparoscopic Ladd Procedure: Case Report and Literature ReviewHendry JohannesNo ratings yet
- Kayatsha - Gastroschisis and Omphalocele A Case ReportDocument4 pagesKayatsha - Gastroschisis and Omphalocele A Case ReportAffannul HakimNo ratings yet
- Ruiz, P. - SGD and NCP On Imperforate AnusDocument8 pagesRuiz, P. - SGD and NCP On Imperforate AnusPatricia Dianne RuizNo ratings yet
- Wood 2018Document10 pagesWood 2018dewaprasatyaNo ratings yet
- Apple Peel Small Bowel, A Review of Four Cases: Surgical and Radiographic AspectsDocument8 pagesApple Peel Small Bowel, A Review of Four Cases: Surgical and Radiographic AspectsraecmyNo ratings yet
- Jurnal MAR 2Document10 pagesJurnal MAR 2Taufik HidayatNo ratings yet
- 1 s2.0 S2049080121010074 MainDocument4 pages1 s2.0 S2049080121010074 Maintithania insanilahiaNo ratings yet
- MRI Findings in Fetuses With An Abdominal Wall Defect: Gastroschisis, Omphalocele, and Cloacal ExstrophyDocument7 pagesMRI Findings in Fetuses With An Abdominal Wall Defect: Gastroschisis, Omphalocele, and Cloacal ExstrophyIngrid TanasaNo ratings yet
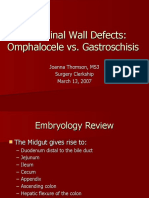
- Abdominal Wall Defects: Omphalocele vs. GastroschisisDocument15 pagesAbdominal Wall Defects: Omphalocele vs. GastroschisisSerag MonierNo ratings yet
- Campbell - Walsh-Wein UROLOGY 12th Ed ADocument6 pagesCampbell - Walsh-Wein UROLOGY 12th Ed Awijana410No ratings yet
- RLQ PainDocument20 pagesRLQ PainBEATRICE SOPHIA PARMANo ratings yet
- Anal AtresiaDocument13 pagesAnal AtresiaAhmad IhsanNo ratings yet
- Intestinal Malrotation and Volvulus: Luisa Ferrero, François Becmeur, and Olivier ReinbergDocument15 pagesIntestinal Malrotation and Volvulus: Luisa Ferrero, François Becmeur, and Olivier ReinbergIván Castellares RojasNo ratings yet
- SigmoidDocument4 pagesSigmoidFKUPR 2017No ratings yet
- Ileal Atresia ReferenceDocument50 pagesIleal Atresia ReferenceOvamelia JulioNo ratings yet
- Developmental Dysplasia of HipDocument13 pagesDevelopmental Dysplasia of HipIndra Purwanto AkbarNo ratings yet
- Review Article: Splenic Anomalies of Shape, Size, and Location: Pictorial EssayDocument10 pagesReview Article: Splenic Anomalies of Shape, Size, and Location: Pictorial EssayyurikepratiwiNo ratings yet
- Surgical Treatment of Anorectal MalformationsDocument8 pagesSurgical Treatment of Anorectal MalformationsGerii Pucllas VillarNo ratings yet
- Obgy 15 3 8Document4 pagesObgy 15 3 8IcicNo ratings yet
- Volvulus: Carol K. Le Phillip Nahirniak Sachit Anand Wantzy Cooper. Author InformationDocument22 pagesVolvulus: Carol K. Le Phillip Nahirniak Sachit Anand Wantzy Cooper. Author InformationMon DoceNo ratings yet
- Ocluzie Intestinala Prin Stenoza Extrinseca de Colon TransversDocument8 pagesOcluzie Intestinala Prin Stenoza Extrinseca de Colon TransversClaudia DanielaNo ratings yet
- OBGYN1222 Core ObstetricsDocument4 pagesOBGYN1222 Core ObstetricsalaiNo ratings yet
- Congenital Aganglionic Megacolon (Hirschsprung Disease) : Kristin N. Fiorino and Chris A. LiacourasDocument6 pagesCongenital Aganglionic Megacolon (Hirschsprung Disease) : Kristin N. Fiorino and Chris A. LiacourasSyakilla AuliaNo ratings yet
- The Disappearing Abdominal Mass: Mesenteric Pseudocyst: Jasneet Singh Bhullar, MD, MS, Paraskevi Orfanou, MDDocument4 pagesThe Disappearing Abdominal Mass: Mesenteric Pseudocyst: Jasneet Singh Bhullar, MD, MS, Paraskevi Orfanou, MDDiyah SeptiRiyantiNo ratings yet
- Soleimani 2007Document9 pagesSoleimani 2007ceciliaNo ratings yet
- From Functional Imaging in Nephro-Urology (Alain Prigent Etc.) (Z-Library)Document10 pagesFrom Functional Imaging in Nephro-Urology (Alain Prigent Etc.) (Z-Library)Francisco BotelhoNo ratings yet
- Anorectal MalformationDocument29 pagesAnorectal Malformationbimaindra97No ratings yet
- Abdominal Wall DefectsDocument14 pagesAbdominal Wall Defectsskeebs23No ratings yet
- Gastroschisis: Etiology, Diagnosis, Delivery Options, and CareDocument6 pagesGastroschisis: Etiology, Diagnosis, Delivery Options, and CareCarolina TorresNo ratings yet
- Title: A Case Report On Left-Sided AppendicitisDocument10 pagesTitle: A Case Report On Left-Sided Appendicitishom lakshmiNo ratings yet
- A Burjonrappa 2011Document6 pagesA Burjonrappa 2011FernandoNo ratings yet
- Imaging Patients With Acute Abdominal PainDocument16 pagesImaging Patients With Acute Abdominal PainNaelul IzahNo ratings yet
- Laparoscopic Splenectomy For Pediatric Wandering Spleen - A Case ReportDocument11 pagesLaparoscopic Splenectomy For Pediatric Wandering Spleen - A Case ReportAdlyn Bea Albesa-BernaldezNo ratings yet
- Abdominal Cystic Disease of The Neonate - A Systematic ReviewDocument6 pagesAbdominal Cystic Disease of The Neonate - A Systematic Reviewtsehayealem12No ratings yet
- Hip Disorders in Children: Postgraduate Orthopaedics SeriesFrom EverandHip Disorders in Children: Postgraduate Orthopaedics SeriesRating: 3 out of 5 stars3/5 (2)
- Tantangan Organisasi Rumah Sakit Masa MendatangDocument17 pagesTantangan Organisasi Rumah Sakit Masa MendatangTanwirul JojoNo ratings yet
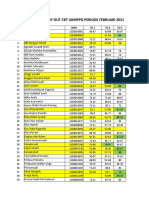
- Rekap Nilai Try Out Februari 2021Document4 pagesRekap Nilai Try Out Februari 2021Tanwirul JojoNo ratings yet
- Imaging Diagnosis of Pancreatic Cancer: A State-Of-The-Art ReviewDocument15 pagesImaging Diagnosis of Pancreatic Cancer: A State-Of-The-Art ReviewTanwirul JojoNo ratings yet
- E-Ticket: Departure FlightDocument2 pagesE-Ticket: Departure FlightTanwirul JojoNo ratings yet
- Mahadevan, V. (2017) - Anatomy of The Stomach. Surgery (Oxford)Document4 pagesMahadevan, V. (2017) - Anatomy of The Stomach. Surgery (Oxford)anastasijaNo ratings yet
- Surgery Illustrated - Surgical Atlas: Mainz Pouch Continent Cutaneous DiversionDocument25 pagesSurgery Illustrated - Surgical Atlas: Mainz Pouch Continent Cutaneous DiversionAbdullah Bangwar100% (1)
- Screening Cancer Ibd PDFDocument8 pagesScreening Cancer Ibd PDFm_manuela2002No ratings yet
- Pathophysiology ExaminationDocument6 pagesPathophysiology ExaminationPractice Medi-nursingNo ratings yet
- Colorectal Cancer PDFDocument2 pagesColorectal Cancer PDFElizabeth100% (1)
- Dr. Murali Bharadwaz Classes For MD/MS Entrance Coaching ProgrammeDocument20 pagesDr. Murali Bharadwaz Classes For MD/MS Entrance Coaching ProgrammeskNo ratings yet
- ProbioticsDocument30 pagesProbioticstummalapalli venkateswara rao100% (2)
- Abdomen AssessmentDocument29 pagesAbdomen AssessmentWawan HediyantoNo ratings yet
- Liver Pathophysiology and Schematic DiagramDocument1 pageLiver Pathophysiology and Schematic DiagramCyrus De Asis100% (4)
- WHS PR Symposium - Non-Alcoholic Fatty Liver DiseaseDocument63 pagesWHS PR Symposium - Non-Alcoholic Fatty Liver DiseaseWomen's Health SocietyNo ratings yet
- Guava Intro 1Document4 pagesGuava Intro 1Thean MendozaNo ratings yet
- Pathophysiology of CholelithiasisDocument2 pagesPathophysiology of CholelithiasisSherilNo ratings yet
- Vitamin B12 Deficiency and A Patient Case StudyDocument36 pagesVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- Case SummaryDocument18 pagesCase SummaryFaryal UfaqNo ratings yet
- Peptic Ulcer HDocument6 pagesPeptic Ulcer HIlyes FerenczNo ratings yet
- Colorectal SurgeryDocument8 pagesColorectal SurgeryGeramyl Ramos AnapiNo ratings yet
- Surgery MnemonicsDocument6 pagesSurgery MnemonicsMarkoMilivojevic50% (2)
- Mini Case Study PresentationDocument19 pagesMini Case Study Presentationapi-537434972No ratings yet
- Case 18Document23 pagesCase 18Hazel Mae SagorsorNo ratings yet
- Discharge PlanDocument5 pagesDischarge PlanrraksNo ratings yet
- BAVENO VII Concept of Cirrhodid RecompensationDocument11 pagesBAVENO VII Concept of Cirrhodid RecompensationValentina IorgaNo ratings yet
- Emergency Medicine: Acute AbdomenDocument33 pagesEmergency Medicine: Acute AbdomenPrashant MishraNo ratings yet
- MS Sas 3Document4 pagesMS Sas 3rereNo ratings yet
- Komi Classification of Bile Duct CystsDocument3 pagesKomi Classification of Bile Duct Cystsmero1983No ratings yet
- Chinese Reflexology Foot ChartsDocument1 pageChinese Reflexology Foot ChartsRaquel Sacramento100% (1)
- Management of Lower GI BleedDocument48 pagesManagement of Lower GI BleedMegat Mohd Azman Adzmi100% (1)
- Psyllium Husk Is Used To Help Support Digestive HealthDocument3 pagesPsyllium Husk Is Used To Help Support Digestive Healthlen castilloNo ratings yet
- Shat KarmaDocument3 pagesShat KarmaMisterNo ratings yet
- Abdominal Pain DischargeDocument2 pagesAbdominal Pain Dischargemfa40No ratings yet
- Vomiting in Children 2018 PDFDocument19 pagesVomiting in Children 2018 PDFSamuel DiazNo ratings yet