You might also like
- 2.1.1 Ebers-Moll Model: 2.1 Introduction To Differential AmpDocument38 pages2.1.1 Ebers-Moll Model: 2.1 Introduction To Differential AmpDiane AlmarioNo ratings yet
- ClassDocument35 pagesClassSrikkanth RamachandranNo ratings yet
- ELNModule 4Document20 pagesELNModule 4Fariya TasneemNo ratings yet
- E) EA 0.01-0.05 V: Semicnductor Lattice, and Hence of HolesDocument10 pagesE) EA 0.01-0.05 V: Semicnductor Lattice, and Hence of HolesDebrup GhoshNo ratings yet
- A New Circuit Design of Two-Switch Buck-Boost ConvDocument10 pagesA New Circuit Design of Two-Switch Buck-Boost ConvBinh NguyenNo ratings yet
- CHAPTER 1 Analysis and Design of Biasing CircuitsDocument62 pagesCHAPTER 1 Analysis and Design of Biasing CircuitsVinod RajanNo ratings yet
- Duarte ECE005 Assignment No.1 PrelimDocument5 pagesDuarte ECE005 Assignment No.1 PrelimJohn Paul DirayNo ratings yet
- Biomedical Sensors Biomedical Sensors: Intro. To. BME Intro. To. BMEDocument67 pagesBiomedical Sensors Biomedical Sensors: Intro. To. BME Intro. To. BMEfaten emadNo ratings yet
- Assignment FET 2Document3 pagesAssignment FET 2shobanraj1995No ratings yet
- Study of DiodeDocument3 pagesStudy of DiodeSai pavanNo ratings yet
- EN2017031061Document2 pagesEN2017031061marcoNo ratings yet
- Potencia PDFDocument109 pagesPotencia PDFdavidNo ratings yet
- Unit 3 - Analog Circuits - WWW - Rgpvnotes.inDocument60 pagesUnit 3 - Analog Circuits - WWW - Rgpvnotes.inRahul kumar singhNo ratings yet
- Ec8453-Linear Integrated Circuits-1451692048-Lic Notes Ec8453Document131 pagesEc8453-Linear Integrated Circuits-1451692048-Lic Notes Ec8453Dr.T.sivakami biherNo ratings yet
- DC To DC Buck and Boost ConverterDocument5 pagesDC To DC Buck and Boost ConverterR ABHISHEKNo ratings yet
- Dependent SourcesDocument11 pagesDependent SourcesM Sadiq Khan NasarNo ratings yet
- Adaptive Voltage PositioningDocument7 pagesAdaptive Voltage PositioningadolfNo ratings yet
- By Anshuman Shukla October 27th, 2007Document27 pagesBy Anshuman Shukla October 27th, 2007ShikhaNeeraj AggarwalNo ratings yet
- 11-BJT DC Characteristics and Analysis-20!02!2024Document15 pages11-BJT DC Characteristics and Analysis-20!02!2024ashbinny1No ratings yet
- Electronic Devices and Circuit Theory Prelim LectureDocument128 pagesElectronic Devices and Circuit Theory Prelim LectureJustin ValdezNo ratings yet
- Baki Ali Neft MəktəbiDocument18 pagesBaki Ali Neft MəktəbiFerid AslanliNo ratings yet
- Experiment NoDocument54 pagesExperiment Nohemant rathodNo ratings yet
- 5.BJT Small Signal Analysis - Part1Document52 pages5.BJT Small Signal Analysis - Part1Hafzn HashimNo ratings yet
- Tunnel DiodeDocument56 pagesTunnel DiodeNaveed Ramzan100% (2)
- LED Flasher Circuit ExplanationDocument5 pagesLED Flasher Circuit ExplanationBharathNo ratings yet
- Module 2 - PPT - Expanded Hybrid Pie Equivalent and Short Circuit Current Gain PDFDocument16 pagesModule 2 - PPT - Expanded Hybrid Pie Equivalent and Short Circuit Current Gain PDFGokulnath SNo ratings yet
- EEE111 - Lab ManualDocument28 pagesEEE111 - Lab ManualAnindita MishiNo ratings yet
- BJT Transistor Modelling: Prepared By: Engr. Mark S. CañeteDocument26 pagesBJT Transistor Modelling: Prepared By: Engr. Mark S. CañeteJanZkie17No ratings yet
- Ecdnotes Part1Document61 pagesEcdnotes Part1ezekiel makandwaNo ratings yet
- UJT CharacteristicsDocument3 pagesUJT CharacteristicsmanasaNo ratings yet
- DC-DC Converter Implementation With Wide Output Voltage OperationDocument12 pagesDC-DC Converter Implementation With Wide Output Voltage OperationsaptadipNo ratings yet
- Op AmpApplicationsDocument10 pagesOp AmpApplicationssrinureddy2014No ratings yet
- EDC Lab ManualDocument63 pagesEDC Lab Manualranjitha gavniNo ratings yet
- LAB 1 Op AmpDocument11 pagesLAB 1 Op AmpamirulNo ratings yet
- 2054359797-BASIC ELNS-UNIT-1 NOTES-DiodesDocument18 pages2054359797-BASIC ELNS-UNIT-1 NOTES-Diodesajey002hegdeNo ratings yet
- Experiment 5 Diodes and DC Power Supplies: Part 1: Diode CharacteristicsDocument4 pagesExperiment 5 Diodes and DC Power Supplies: Part 1: Diode CharacteristicsrishavNo ratings yet
- Online - Bai 2 - Mach Ban DanDocument15 pagesOnline - Bai 2 - Mach Ban DanThất VọngNo ratings yet
- Unit 1 Intro To Op AmpDocument31 pagesUnit 1 Intro To Op AmpKrishna RamaNo ratings yet
- Effect of Supply Voltage On Output VoltageDocument5 pagesEffect of Supply Voltage On Output VoltageMahammad HaneefNo ratings yet
- A ZVS DC-DC Converter Based On Buck Topology: Qiang Tong, Nanxiao Zhong, Mingsheng Yang and Donglai ZhangDocument4 pagesA ZVS DC-DC Converter Based On Buck Topology: Qiang Tong, Nanxiao Zhong, Mingsheng Yang and Donglai ZhangsuneelNo ratings yet
- Unit IiiDocument16 pagesUnit Iiikannan305No ratings yet
- Transistor CharacteristicsDocument44 pagesTransistor Characteristicsnidhi100% (1)
- EXPERIMENT No 4Document3 pagesEXPERIMENT No 4English words BY Utkarsh johriNo ratings yet
- Laboratory Report Cover Sheet: 21Ecc211L - Devices and Digital Ic Lab Third Semester, 2023-24 (Odd Semester)Document12 pagesLaboratory Report Cover Sheet: 21Ecc211L - Devices and Digital Ic Lab Third Semester, 2023-24 (Odd Semester)nikunj sharmaNo ratings yet
- 3.1 BJTransistors pt1 Rev2.3 LectDocument37 pages3.1 BJTransistors pt1 Rev2.3 LectShudermawan JarumanNo ratings yet
- Electronic Devices & Circuits (EDC) PE-124: Prepared By: Engr. Shafaq EjazDocument19 pagesElectronic Devices & Circuits (EDC) PE-124: Prepared By: Engr. Shafaq EjazShafaq EjazNo ratings yet
- Basic Electro - Module 3 - KtuQbankDocument21 pagesBasic Electro - Module 3 - KtuQbankveenau 1No ratings yet
- RESEARCH of Communications Research No. 2Document19 pagesRESEARCH of Communications Research No. 2Princess EsmejardaNo ratings yet
- Electronic Devices Ch2 Part1Document20 pagesElectronic Devices Ch2 Part1ahmad kakiNo ratings yet
- Section F4: Power Amplifier Circuits - Class B & AB: Complementary Symmetry) ConfigurationDocument8 pagesSection F4: Power Amplifier Circuits - Class B & AB: Complementary Symmetry) ConfigurationKiệt NgôNo ratings yet
- LIC Lecture 3-Current Sources As Active Loads and Voltage Sources MaterialsDocument4 pagesLIC Lecture 3-Current Sources As Active Loads and Voltage Sources MaterialsMadhavan SamNo ratings yet
- Experiment # 2 (Final)Document11 pagesExperiment # 2 (Final)John Mickelson FaustinoNo ratings yet
- Solid States Final TestDocument7 pagesSolid States Final TestRickel RoweNo ratings yet
- Module 1Document21 pagesModule 1yakomi suraNo ratings yet
- An Active Damping Strategy For Input Impedance of Bidirectional Dual Active Bridge DC-DC Converter: Modelling, Shaping, Design, and ExperimentDocument12 pagesAn Active Damping Strategy For Input Impedance of Bidirectional Dual Active Bridge DC-DC Converter: Modelling, Shaping, Design, and ExperimentJaja LocoNo ratings yet
- A Single Phase DC-AC Dual Active Bridge Series Resonant Converter For Photovoltaic ApplicationsDocument6 pagesA Single Phase DC-AC Dual Active Bridge Series Resonant Converter For Photovoltaic ApplicationsDEBARATI DAMNo ratings yet
- Lecture - BJT AC-AnalysisDocument43 pagesLecture - BJT AC-AnalysisAdam MoutasemNo ratings yet
- Easy(er) Electrical Principles for General Class Ham License (2019-2023)From EverandEasy(er) Electrical Principles for General Class Ham License (2019-2023)No ratings yet
- Diss PDFDocument168 pagesDiss PDFCarlos Manuel Carranza VegaNo ratings yet
- TD AlbertoLopezMartinez PDFDocument286 pagesTD AlbertoLopezMartinez PDFCarlos Manuel Carranza VegaNo ratings yet
- 3264.TI ECG Fundamentals Condensed v08 PDFDocument105 pages3264.TI ECG Fundamentals Condensed v08 PDFCarlos Manuel Carranza VegaNo ratings yet
- MicromouseDocument7 pagesMicromouseCarlos Manuel Carranza VegaNo ratings yet
- Futura V1.1 SchematicDocument20 pagesFutura V1.1 SchematicCarlos Manuel Carranza VegaNo ratings yet
- Futura V1.1 Schematic PDFDocument1 pageFutura V1.1 Schematic PDFCarlos Manuel Carranza VegaNo ratings yet
- Hiv and PregnancyDocument7 pagesHiv and PregnancyCarlos Manuel Carranza VegaNo ratings yet
- Neurodesarrollo PEG Japón 2015Document9 pagesNeurodesarrollo PEG Japón 2015Carlos Manuel Carranza VegaNo ratings yet
- Oftalmologia PracticaDocument5 pagesOftalmologia PracticaCarlos Manuel Carranza VegaNo ratings yet
- Nasopharyngeal Angiofibroma - PPTX Essam SrourDocument10 pagesNasopharyngeal Angiofibroma - PPTX Essam SrourSimina ÎntunericNo ratings yet
- Market AnalysisDocument4 pagesMarket AnalysisSaniya CharaniyaNo ratings yet
- Board Replacement CasesDocument41 pagesBoard Replacement CasesNadeeshNo ratings yet
- Tree Growth CharacteristicsDocument9 pagesTree Growth CharacteristicsMunganNo ratings yet
- Dawn of Solar PV CookingDocument5 pagesDawn of Solar PV CookingAbhinav AgrawalNo ratings yet
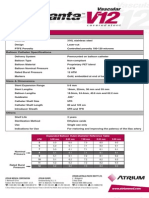
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiNo ratings yet
- Inferring The Speaker's Tone, ModeDocument31 pagesInferring The Speaker's Tone, Modeblessilda.delaramaNo ratings yet
- Cynosure Starlux 500 Palomar Technical Service ManualDocument47 pagesCynosure Starlux 500 Palomar Technical Service ManualJF SilvaNo ratings yet
- Effects of Climate ChangeDocument3 pagesEffects of Climate Changejiofjij100% (1)
- Goldhofer FTV 850 BrochureDocument2 pagesGoldhofer FTV 850 BrochureMauroNo ratings yet
- Scanner and Xcal Comperative Analysis v2Document22 pagesScanner and Xcal Comperative Analysis v2Ziya2009No ratings yet
- Plastics and Polymer EngineeringDocument4 pagesPlastics and Polymer Engineeringsuranjana26No ratings yet
- Arbor APS STT Unit 01 Design Basics 25 Jan2018Document31 pagesArbor APS STT Unit 01 Design Basics 25 Jan2018masterlinh2008No ratings yet
- ZF-FreedomLine TransmissionDocument21 pagesZF-FreedomLine TransmissionHerbert M. Zayco100% (1)
- Pediatric EmergenciesDocument47 pagesPediatric EmergenciesahmedNo ratings yet
- Flight Vehicle Design:: Example 2 (Uav)Document43 pagesFlight Vehicle Design:: Example 2 (Uav)Anmol KumarNo ratings yet
- Dual Shield 7100 Ultra: Typical Tensile PropertiesDocument3 pagesDual Shield 7100 Ultra: Typical Tensile PropertiesDino Paul Castro HidalgoNo ratings yet
- Soldier of Fortune PDFDocument208 pagesSoldier of Fortune PDFNixel SpielNo ratings yet
- OurCatholicFaith PowerPoint Chapter1Document21 pagesOurCatholicFaith PowerPoint Chapter1VinNo ratings yet
- Tugas 2-TRK Lanjut Kelompok 3 Andre-Arief-IstiaDocument18 pagesTugas 2-TRK Lanjut Kelompok 3 Andre-Arief-IstiaAndre Fahriz Perdana HarahapNo ratings yet
- SCM (Subway Project Report)Document13 pagesSCM (Subway Project Report)Beast aNo ratings yet
- Kinematics in One DimensionDocument4 pagesKinematics in One DimensionAldrin VillanuevaNo ratings yet
- Ali Erdemir: Professional ExperienceDocument3 pagesAli Erdemir: Professional ExperienceDunkMeNo ratings yet
- DMDWLab Book AnswersDocument44 pagesDMDWLab Book AnswersNarpat Makwana Pune100% (1)
- American BreakfastDocument4 pagesAmerican BreakfastHamilton Valenzuela ChipongianNo ratings yet
- The Broadband ForumDocument21 pagesThe Broadband ForumAnouar AleyaNo ratings yet
- DudjDocument4 pagesDudjsyaiful rinantoNo ratings yet
- 41z S4hana2021 Set-Up en XXDocument46 pages41z S4hana2021 Set-Up en XXHussain MulthazimNo ratings yet
- Determinants - DPP 01 (Of Lec 02) - Lakshya JEE 2.0 2024Document3 pagesDeterminants - DPP 01 (Of Lec 02) - Lakshya JEE 2.0 2024Apurv ChitranshNo ratings yet
- G1CDocument12 pagesG1CKhriz Ann C ÜNo ratings yet