You might also like
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsFrom EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNo ratings yet
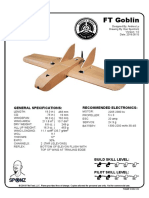
- FT Goblin Full SizeDocument7 pagesFT Goblin Full SizeDeakon Frost100% (1)
- Control of Documented Information Procedure SampleDocument4 pagesControl of Documented Information Procedure Sampleingventor0% (1)
- Bernardo Corporation Statement of Financial Position As of Year 2019 AssetsDocument3 pagesBernardo Corporation Statement of Financial Position As of Year 2019 AssetsJean Marie DelgadoNo ratings yet
- Ata 36 PDFDocument149 pagesAta 36 PDFAyan Acharya100% (2)
- MsgSpec v344 PDFDocument119 pagesMsgSpec v344 PDFqweceNo ratings yet
- PNA Summer Conference RegistrationDocument1 pagePNA Summer Conference RegistrationMario Oracion Jr.No ratings yet
- Offshore Medic Course Registration FormDocument2 pagesOffshore Medic Course Registration FormRoyal Experience (RXp)No ratings yet
- ApplicationFormSY2018 2019 (SHS) PDFDocument15 pagesApplicationFormSY2018 2019 (SHS) PDFAngelicaNo ratings yet
- 286th Bosh DavaoDocument2 pages286th Bosh DavaoKaren BugingNo ratings yet
- ApplicationFormSY2023-2024SHSDocument15 pagesApplicationFormSY2023-2024SHSjamesporton134No ratings yet
- FTRA Form 2 RenewalDocument3 pagesFTRA Form 2 RenewalNimiloteNo ratings yet
- Chiropractic Application Form: Section A: Contact InformationDocument6 pagesChiropractic Application Form: Section A: Contact InformationAmanakeNo ratings yet
- Occupational Health Nurses Association of The Philippines (Ohnap), IncDocument2 pagesOccupational Health Nurses Association of The Philippines (Ohnap), IncRalph Roentgen Diwa ParaguisonNo ratings yet
- PUPSARForm2018 0002 1435Document5 pagesPUPSARForm2018 0002 1435ethelfajardoNo ratings yet
- FE-application-form For Upload PDFDocument2 pagesFE-application-form For Upload PDFJohn JardelozaNo ratings yet
- FE Application Form For UploadDocument2 pagesFE Application Form For Upload1234qwertyNo ratings yet
- NCNZ1 Employment Validation FormDocument3 pagesNCNZ1 Employment Validation FormEmma IntiaNo ratings yet
- OJT-Application-formDocument3 pagesOJT-Application-formSayong , John Mike J.No ratings yet
- Important Reminders for Your Upcoming Passport AppointmentDocument4 pagesImportant Reminders for Your Upcoming Passport AppointmentKeith MedinaNo ratings yet
- Adpcn Membership Form 2018Document2 pagesAdpcn Membership Form 2018Vivi rikka100% (3)
- 1st Annual CARD Conference Reservation FormDocument1 page1st Annual CARD Conference Reservation Formvictoria chavezNo ratings yet
- ADNEP 8th Joint Annual Convention of PADE and ADNEP Registration PaperDocument1 pageADNEP 8th Joint Annual Convention of PADE and ADNEP Registration PaperPhilippineNursingDirectory.comNo ratings yet
- New Membership Form 2019 Ver 0.6 Fillable FormDocument1 pageNew Membership Form 2019 Ver 0.6 Fillable FormcaffeinatedrmtNo ratings yet
- Directions: Fill-Up by Putting A Check Mark (/) On The Appropriate Box or by Writing The Needed Information. Please Write LegiblyDocument2 pagesDirections: Fill-Up by Putting A Check Mark (/) On The Appropriate Box or by Writing The Needed Information. Please Write LegiblyJen BatiagaoNo ratings yet
- Incident Investigation & Root Cause Analysis Implementation: Registration FormDocument2 pagesIncident Investigation & Root Cause Analysis Implementation: Registration FormKotiti PhilippinesNo ratings yet
- Requirement Medical Report Form3Document1 pageRequirement Medical Report Form3KUMAR LOKESHNo ratings yet
- 2024-2025 Hmo Advisory & EnrollmentDocument14 pages2024-2025 Hmo Advisory & EnrollmentJona ReyesNo ratings yet
- Training Form PDFDocument4 pagesTraining Form PDF2013alexizoNo ratings yet
- Adventist College of Nursing & Health Sciences, Penang: For Office Use OnlyDocument3 pagesAdventist College of Nursing & Health Sciences, Penang: For Office Use OnlyCarthieca tiecacueNo ratings yet
- SGP Generic Claim FormDocument5 pagesSGP Generic Claim FormSanny HamdaniNo ratings yet
- Association of Deans of Philippine Colleges of Nursing, Inc. (ADPCN, Inc.)Document2 pagesAssociation of Deans of Philippine Colleges of Nursing, Inc. (ADPCN, Inc.)Jefferyi Knigth AlVarezNo ratings yet
- Registration FormDocument2 pagesRegistration Formshannonie8No ratings yet
- Metropolitan PharmaceuticalDocument3 pagesMetropolitan Pharmaceuticalcopy pacific valNo ratings yet
- Registration Form For Promotional Bundle For 1 Trainor and 2 TraineesDocument1 pageRegistration Form For Promotional Bundle For 1 Trainor and 2 TraineesJenny Calapati TorrijosNo ratings yet
- Registration Form For Promotional Bundle For 1 Trainor and 2 TraineesDocument1 pageRegistration Form For Promotional Bundle For 1 Trainor and 2 TraineesJenny Calapati TorrijosNo ratings yet
- Registration Form For Promotional Bundle For 1 Trainor and 2 TraineesDocument1 pageRegistration Form For Promotional Bundle For 1 Trainor and 2 TraineesJenny Calapati TorrijosNo ratings yet
- Application 2011Document2 pagesApplication 2011laltea2677No ratings yet
- Philippine National Police Academy: Cadet Admission Test Application FormDocument4 pagesPhilippine National Police Academy: Cadet Admission Test Application FormRussel GuntangNo ratings yet
- 2example For Fill Up 1Document4 pages2example For Fill Up 1angeloworkacc16No ratings yet
- Important RemindersDocument4 pagesImportant RemindersSpencer Phay VillalunaNo ratings yet
- F57 050221 Indigency Form1Document1 pageF57 050221 Indigency Form1Gideon HidalgoNo ratings yet
- Continuing Education: Course Registration FormDocument1 pageContinuing Education: Course Registration FormGurkirtanNo ratings yet
- Ku Postgraduate Scholarships Application Form 2019Document2 pagesKu Postgraduate Scholarships Application Form 2019Apoll BillyNo ratings yet
- CHED Authentication FormDocument1 pageCHED Authentication FormMarilou PagalaNo ratings yet
- ABC Biomedical Seminar on Medical Equipment SafetyDocument2 pagesABC Biomedical Seminar on Medical Equipment Safetyver_at_workNo ratings yet
- Form A - Consent Form SGH - NATIONAL CANCER CENTER SINGAPOREDocument1 pageForm A - Consent Form SGH - NATIONAL CANCER CENTER SINGAPOREChika KhakaNo ratings yet
- F-HCA-041 Member and Card Maintenance Form r3Document1 pageF-HCA-041 Member and Card Maintenance Form r3christina loNo ratings yet
- Maxicare Maintenance FormDocument1 pageMaxicare Maintenance FormEdd Nysha ManguilimotanNo ratings yet
- Verification of Nursing PracticeDocument2 pagesVerification of Nursing PracticewilliamshenoyNo ratings yet
- ACCP Registration FormDocument2 pagesACCP Registration FormKlub 'Apoteker' IndonesiaNo ratings yet
- Form Must Be Returned Within 15 Days. Parts 1-3 Must Be Completed For The Application To Be ApprovedDocument1 pageForm Must Be Returned Within 15 Days. Parts 1-3 Must Be Completed For The Application To Be ApprovedKenneth SandersNo ratings yet
- PCU Ministerial Scholarship ApplicationDocument15 pagesPCU Ministerial Scholarship ApplicationChristian Cyril EspenillaNo ratings yet
- Health Insurance Claim FormDocument3 pagesHealth Insurance Claim FormdivechahimanshuNo ratings yet
- Letter of Intent: (Given Name, Middle Name, Surname)Document1 pageLetter of Intent: (Given Name, Middle Name, Surname)Shaira AgulanNo ratings yet
- 2023 Pfa Allied Membership Application FormDocument2 pages2023 Pfa Allied Membership Application FormJohn OcamposNo ratings yet
- 30 Medicl Procdur For ClaimDocument7 pages30 Medicl Procdur For Claimبلال خالدNo ratings yet
- Important RemindersDocument4 pagesImportant RemindersMacky BirdNo ratings yet
- NIAT International Certification ApplicationDocument1 pageNIAT International Certification ApplicationChing MaderazoNo ratings yet
- Case Form PRC BSNDocument5 pagesCase Form PRC BSNCarol Neng CalupitanNo ratings yet
- Application Form 2Document2 pagesApplication Form 2Scott VerosilNo ratings yet
- Forman Christian College: (A Chartered University) Financial Aid Provisional Assessment FormDocument2 pagesForman Christian College: (A Chartered University) Financial Aid Provisional Assessment Formraza haiderNo ratings yet
- Medical Group: 1-888-236-2263. Our Office Hours Are Monday Through Friday 8:00a.m.to 4:30p.mDocument3 pagesMedical Group: 1-888-236-2263. Our Office Hours Are Monday Through Friday 8:00a.m.to 4:30p.menergizerabbyNo ratings yet
- Verification of RegistrationDocument2 pagesVerification of RegistrationMETRO SAN JOSE MEDICAL CENTERNo ratings yet
- Academic: Applicant Personal InformationDocument3 pagesAcademic: Applicant Personal InformationShakeel AhmedNo ratings yet
- HGVSJDocument2 pagesHGVSJRhod Bernaldez EstaNo ratings yet
- Statistics PDFDocument54 pagesStatistics PDFRhod Bernaldez EstaNo ratings yet
- Radically Redesigning: Patient SafetyDocument9 pagesRadically Redesigning: Patient SafetyRhod Bernaldez EstaNo ratings yet
- Leadership DevelopmentDocument2 pagesLeadership DevelopmentRhod Bernaldez EstaNo ratings yet
- Carrebean SeaDocument7 pagesCarrebean SeaRhod Bernaldez Esta100% (1)
- Perceive/observe It. Please Answer All Items On This Sheet. If An Item Is Irrelevant, or IfDocument3 pagesPerceive/observe It. Please Answer All Items On This Sheet. If An Item Is Irrelevant, or IfRhod Bernaldez EstaNo ratings yet
- Erastus Perceptions 2018 PDFDocument105 pagesErastus Perceptions 2018 PDFRhod Bernaldez EstaNo ratings yet
- Official Receipt PDFDocument1 pageOfficial Receipt PDFRhod Bernaldez EstaNo ratings yet
- Grenada History, Geography, Politics and EconomyDocument2 pagesGrenada History, Geography, Politics and EconomyRhod Bernaldez EstaNo ratings yet
- Patient Safety Culture in Primary Care: Natasha VerbakelDocument176 pagesPatient Safety Culture in Primary Care: Natasha VerbakelRhod Bernaldez EstaNo ratings yet
- NursingDocument1 pageNursingRhod Bernaldez EstaNo ratings yet
- RHOD Seniority Complex Semi FinalDocument39 pagesRHOD Seniority Complex Semi FinalRhod Bernaldez EstaNo ratings yet
- Patient Safety Incident Reporting - Canadian Health SystemDocument13 pagesPatient Safety Incident Reporting - Canadian Health SystemRhod Bernaldez EstaNo ratings yet
- Sops Hospital Survey: Language: EnglishDocument6 pagesSops Hospital Survey: Language: EnglishNoviyanti LindaNo ratings yet
- Facil Scan FormDocument7 pagesFacil Scan FormJoe ThesecondmonthNo ratings yet
- AHRQ Patient Safety Culture Improvement PlanDocument4 pagesAHRQ Patient Safety Culture Improvement PlanRhod Bernaldez EstaNo ratings yet
- Relationship Between Patient Safety Culture and Safety Outcome Measures Among NursesDocument80 pagesRelationship Between Patient Safety Culture and Safety Outcome Measures Among NursesRhod Bernaldez EstaNo ratings yet
- Patient Safety in Primary Healthcare A Review of The Literature August 2015Document160 pagesPatient Safety in Primary Healthcare A Review of The Literature August 2015Rhod Bernaldez EstaNo ratings yet
- MHD Mission VisionDocument1 pageMHD Mission VisionRhod Bernaldez EstaNo ratings yet
- Gardner-Webb University Digital Commons at Gardner-Webb UniversityDocument132 pagesGardner-Webb University Digital Commons at Gardner-Webb UniversityRhod Bernaldez EstaNo ratings yet
- Objectives 2. Scope 3. Responsibilities 4. Records and References 5. Procedure Details Page No. Rev. No. Effectivity Nature of ChangeDocument8 pagesObjectives 2. Scope 3. Responsibilities 4. Records and References 5. Procedure Details Page No. Rev. No. Effectivity Nature of ChangeRhod Bernaldez EstaNo ratings yet
- Nurses' Perceptions of Patient Safety Culture in Oman: Fatma Al Dhabbari MSC, Pgd. BSC (Hons), R.G.NDocument3 pagesNurses' Perceptions of Patient Safety Culture in Oman: Fatma Al Dhabbari MSC, Pgd. BSC (Hons), R.G.NRhod Bernaldez EstaNo ratings yet
- Perceived Safety Culture of Healthcare Providers in Hospitals in The PhilippinesDocument14 pagesPerceived Safety Culture of Healthcare Providers in Hospitals in The PhilippinesRhod Bernaldez EstaNo ratings yet
- Icrd Vawc-1Document1 pageIcrd Vawc-1Rhod Bernaldez EstaNo ratings yet
- NursingDocument1 pageNursingRhod Bernaldez EstaNo ratings yet
- Fallpxtool 1 BDocument2 pagesFallpxtool 1 BRhod Bernaldez EstaNo ratings yet
- Implementing Rules and Regulations of The Lending Company Regulation Act of 2007 Ra9474Document19 pagesImplementing Rules and Regulations of The Lending Company Regulation Act of 2007 Ra9474Lance DionelaNo ratings yet
- Leadership DevelopmentDocument2 pagesLeadership DevelopmentRhod Bernaldez EstaNo ratings yet
- Law of TortsDocument22 pagesLaw of TortsRadha KrishanNo ratings yet
- Las Q1Document9 pagesLas Q1Gaux SkjsjaNo ratings yet
- Mba Assignment SampleDocument5 pagesMba Assignment Sampleabdallah abdNo ratings yet
- Variable Displacement Closed Circuit: Model 70160 Model 70360Document56 pagesVariable Displacement Closed Circuit: Model 70160 Model 70360michael bossa alisteNo ratings yet
- Wind EnergyDocument6 pagesWind Energyshadan ameenNo ratings yet
- Tokyo Disneyland ItineraryDocument8 pagesTokyo Disneyland ItineraryTayla Allyson ThomasNo ratings yet
- CompactLogix 5480 Controller Sales GuideDocument2 pagesCompactLogix 5480 Controller Sales GuideMora ArthaNo ratings yet
- Haul Cables and Care For InfrastructureDocument11 pagesHaul Cables and Care For InfrastructureSathiyaseelan VelayuthamNo ratings yet
- Introduction To Elective DesignDocument30 pagesIntroduction To Elective Designabdullah 3mar abou reashaNo ratings yet
- For Mail Purpose Performa For Reg of SupplierDocument4 pagesFor Mail Purpose Performa For Reg of SupplierAkshya ShreeNo ratings yet
- Developing a Positive HR ClimateDocument15 pagesDeveloping a Positive HR ClimateDrPurnima SharmaNo ratings yet
- Open Compute Project AMD Motherboard Roadrunner 2.1 PDFDocument36 pagesOpen Compute Project AMD Motherboard Roadrunner 2.1 PDFakok22No ratings yet
- Circular 09/2014 (ISM) : SubjectDocument7 pagesCircular 09/2014 (ISM) : SubjectDenise AhrendNo ratings yet
- Computers As Components 2nd Edi - Wayne WolfDocument815 pagesComputers As Components 2nd Edi - Wayne WolfShubham RajNo ratings yet
- Short Term Training Curriculum Handbook: General Duty AssistantDocument49 pagesShort Term Training Curriculum Handbook: General Duty AssistantASHISH BARAWALNo ratings yet
- Econometrics Chapter 1 7 2d AgEc 1Document89 pagesEconometrics Chapter 1 7 2d AgEc 1Neway AlemNo ratings yet
- Department of Labor: kwc25 (Rev-01-05)Document24 pagesDepartment of Labor: kwc25 (Rev-01-05)USA_DepartmentOfLaborNo ratings yet
- Analytical DataDocument176 pagesAnalytical DataAsep KusnaliNo ratings yet
- Sav 5446Document21 pagesSav 5446Michael100% (2)
- Elementary School: Cash Disbursements RegisterDocument1 pageElementary School: Cash Disbursements RegisterRonilo DagumampanNo ratings yet
- Nature and Effects of ObligationsDocument5 pagesNature and Effects of ObligationsIan RanilopaNo ratings yet
- Civil Aeronautics BoardDocument2 pagesCivil Aeronautics BoardJayson AlvaNo ratings yet
- De Thi Chuyen Hai Duong 2014 2015 Tieng AnhDocument4 pagesDe Thi Chuyen Hai Duong 2014 2015 Tieng AnhHuong NguyenNo ratings yet
- Yamaha Nmax 155 - To Turn The Vehicle Power OffDocument1 pageYamaha Nmax 155 - To Turn The Vehicle Power Offmotley crewzNo ratings yet
- 13-07-01 Declaration in Support of Skyhook Motion To CompelDocument217 pages13-07-01 Declaration in Support of Skyhook Motion To CompelFlorian MuellerNo ratings yet
- Model S-20 High Performance Pressure Transmitter For General Industrial ApplicationsDocument15 pagesModel S-20 High Performance Pressure Transmitter For General Industrial ApplicationsIndra PutraNo ratings yet